By Deepak Natarajan
Tuesday, February 19, 2013
Operator(s):
Deepak Natarajan, Nirmalya Mukherjee and Rohit Kumar.
Affiliation:
Cardiological Society of India.
Facility:
Moolchand MedCity, New Delhi, India
History:
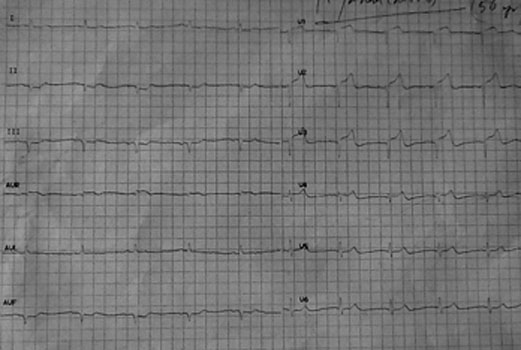
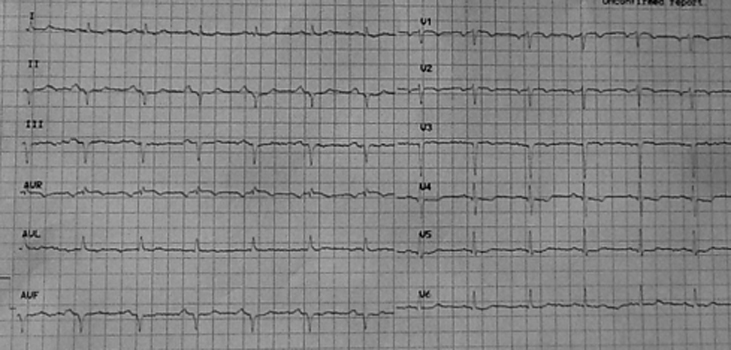
A 56 year male who had been smoking for more than 4 decades and had undergone PCI with stenting of his mid left anterior descending (LAD) artery in 2004 presented with severe retrosternal chest pain with perspiration and breathlessness. His 12 lead ECG revealed sinus rhythm with ST elevation from V1-V3 and ST segment depression in L2, L3, and AVF (Figure 1). The patient had persisted with smoking and had been erratic with his medication.
{kind=link}
Angiography:
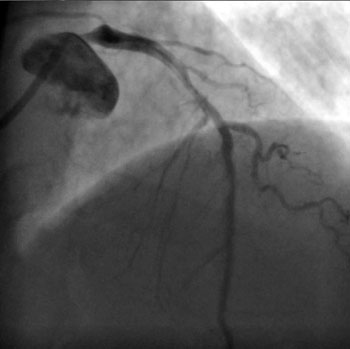
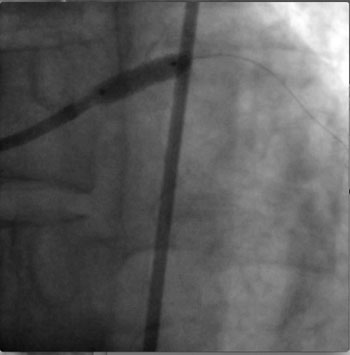
1) RCA: Near normal and dominant and providing collaterals to the left circumflex artery (LCX) (figure 2).
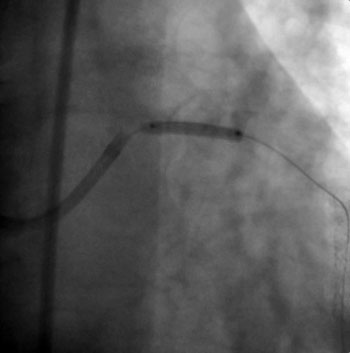
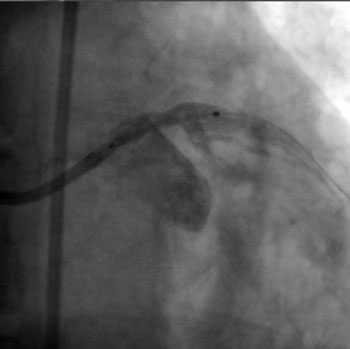
2) LM: 85% ostial stenosis with a 50% stenosis of the proximal LAD. The stent in the LAD was patent. The LCX was totally occluded proximally (figure 3, figure 4 ).
3) The SYNTAX score was calculated at 30 (intermediate risk group).
{kind=link}
{kind=link}
{kind=link}
Procedure:
In view of the acute coronary syndrome setting it was decided to do PCI of the left main lesions. A 0.014″ floppy guidewire was negotiated across the LM lesions into the LAD. The LM lesions were pre-dilated with a 2.5x15mm balloon (figure 5) with the balloon protruding slightly into the aorta. A 3.5x15mm Resolute DES was similarly positioned with slight extension into the aorta and deployed at 16atm (figure 6, figure 7). Post-dilation was performed with a 4.5X12mm NC balloon at 18atm (figure 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Conclusion:
Angiogram demonstrated brisk TIMI 3 flow with no residual stenosis (figure 9, figure 10). There was also rapid resolution in his 12 lead ECG (figure 11).
{kind=link}
{kind=link}
{kind=link}
Comments:
Significant unprotected left main coronary artery stenoses occur in 5-6% of patients undergoing coronary angiography. Meta-analyses have shown similar mortality rates up to one year with CABG and PCI, but repeat revascularization has always been more common with PCI while CVA has always been greater with CABG.
The 5-year results of the SYNTAX trial has showed comparable mortality and myocardial infarction rates in patients with LM disease undergoing CABG and PCI in the low and intermediate SYNTAX score groups. The results were quite different in patients with 3-vessel disease where CABG was superior in the intermediate and high SYNTAX score groups.
This patient had an intermediate risk (SYNTAX) score with lesions of his left main ostium and shaft. Left main disease of the ostium and or body are considered a 2a indication by both European and American interventional cardiology societies. But this patient also had multivessel disease and would therefore fall in the 2b indication slot. Managing ostial/shaft left main disease is relatively simpler than distal left main disease, but care must be taken to ensure that the stent protrudes just a little bit proximally into the aorta. In this case a second generation DES was utilized; it may perform the same or better than the paclitaxel DES used in SYNTAX. The ongoing EXCEL trial compares Xience (everolimus eluting) stents with CABG in patients with left main disease.
In the ACS setting PCI for ULMCA carries an in-hospital mortality rate of almost 20% while death rates have been found to be about 11% in patients with ST-segment elevation myocardial infarction.
Conflict of Interest:
None