By Deepak Natarajan
Monday, April 05, 2010
Operator(s):
Deepak Natarajan, Mriganka Bharali, CK Krishna and Nirmalya Mukherjee
Affiliation:
Moolchand MedCity
New Delhi, India.
Facility:
Department of Interventional Cardiology
Moolchand MedCity
New Delhi, India
History:
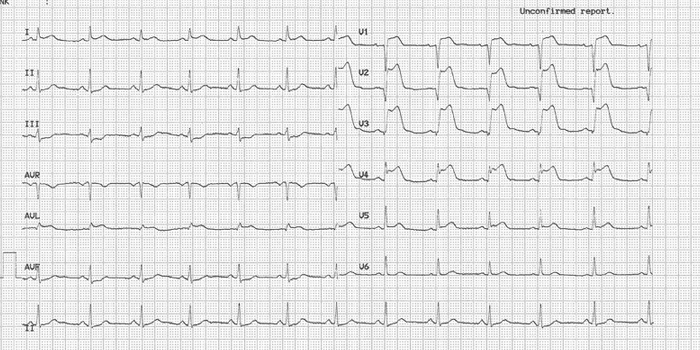
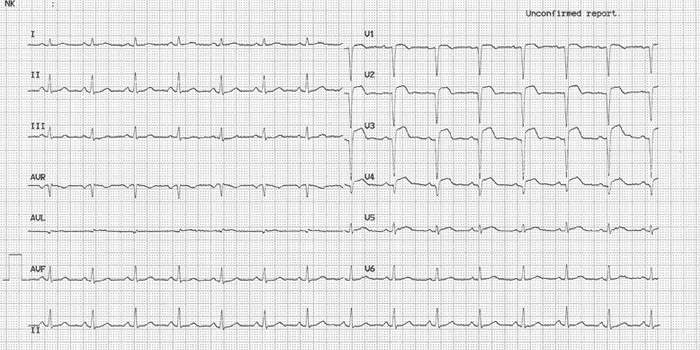
A 50 year old non-diabetic, non hypertensive, and non smoking man was admitted in the emergency with severe chest pain of one hour duration. His 12 lead ECG revealed acute anterior ST elevation myocardial infarction (STEMI) (Figure 1). He had basal crackles and soon began having frequent short runs of ventricular tachycardia that necessitated 2 bulus injections of lignocaine.
{kind=link}
Angiography(via the radial artery):
1) Normal left main
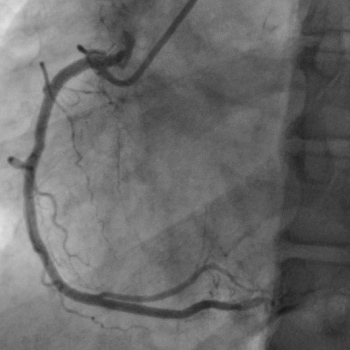
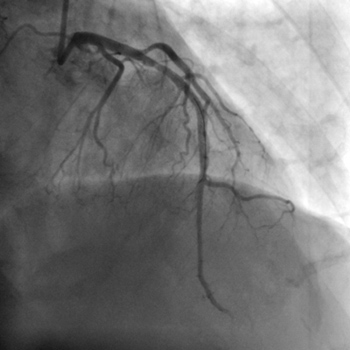
2) Left anterior descending (LAD) Artery totally occluded proximally (Figure 2)
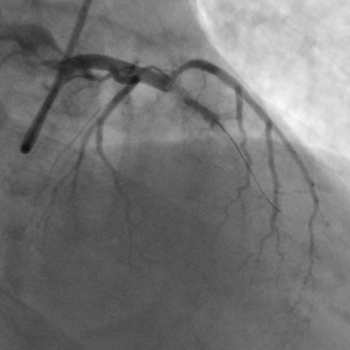
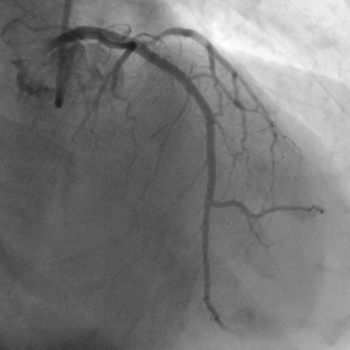
3) Normal left circumflex artery (LCX) (Figure 3)
4) Normal right coronary artery (RCA) (Figure 4)
{kind=link}
{kind=link}
{kind=link}
Procedure:
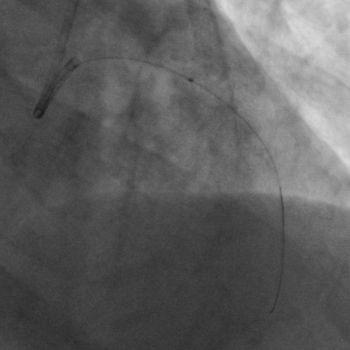
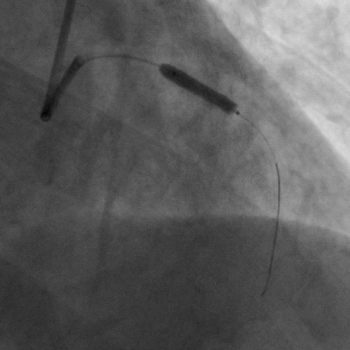
The left coronary artery was engaged by a 6Fr EBU guiding catheter, and a BMW 0.014 inch was initially used to cross the occlusion. The BMW guidewire kept slipping into the diagonal branch adjacent to the LAD occlusion. A CROSS-IT 100 guidewire was subsequently negotiated across the total LAD occlusion, and a bolus of intracoronary (IC) tirofiban was administered in 1 minute (25 mcg/Kg). This was followed by predilation by a 2x12mm balloon (Figure 5). A 6 Fr Export catheter for manual thombus suction was next deployed twice because of significant thrombus burden and sluggish flow following IC rirofiban and predilation (Figure 6, Figure 7). Manual thrombosuction resulted in TIMI 3 flow with minimal residual visible thrombus (Figure 8). The procedure was completed by the deployment of a 3x18mm Yukon DES at 18atm (Figure 9). Brisk TIMI 3 antegrade flow was achieved with no residual stenosis (Figure 10,Figure 11)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Conclusion:
There was rapid disappearance of chest pain with restoration of epicardial LAD blood flow and near complete resolution of ST segment changes in less than 60 minutes suggesting excellent myocardial reperfusion (Figure 12). Intravenous tirofiban was continued for 24 hours; and the patient discharged on 150mg aspirin, 150mg clopidogrel, and 200mg of cilostazol.
{kind=link}
Comments:
There is limited to no data on IC glycoprotein 2b/3a blockers administered in STEMI. A small German randomized study concluded that IC abciximab in STEMI resulted in smaller infarcts, less microvascular obstruction, and better perfusion compared to intravenous abciximab. Another smaller study employing IC eptifibatide in patients with acute coronary syndrome revealed more local receptor occupancy by IC eptifibatide and better microvascular reperfusion. This study did not include patients with STEMI requiring primary PCI. Manual thrombus extraction has been shown by the TAPAS and EXPIRA studies to reduce infarct size and mortality. The technique is safe, effective, and easy to perform.
This case report highlights the need for more randomized studies to establish the synergistic effect of combining IC tirofiban with thrombosuction in patients with STEMI.
The single most effective technique to significantly reduce bleeding at access site is the radial approach which was used in this patient.
Conflict of Interest:
None