By Deepak Natarajan
Monday, February 02, 2009
Operator(s):
Deepak Natarajan, MD, DM and Sandeep Vohra, MD
Affiliation:
Indraprastha Apollo Hospitals,New Delhi
Facility:
Departments of Cardiology
Indraprastha Apollo Hospitals, New Delhi, India
History:
A 47 yr old uncontrolled type 2 diabetic with hypertension and a previous stent in his RCA was admitted for severe intermittent central chest pain for the past 12 hours. He was also having marked shortness of breath. His Troponin T was raised, and the ECG showed ST segment elevations in the anterior leads.
Angiography:
Done by the right radial artery approach using a 6 Fr Terumo sheath and a 6Fr Terumo TIG diagnostic catheter:
LM :OK
LAD: Tight proximal 75% long stenosis with large thrombus burden in the most proximal part of the stenosis 

LCX; Dominant vessel with a proximal ulcerated 85% stenosis 
RCA: Small vessel with patent previous stent in mid segment 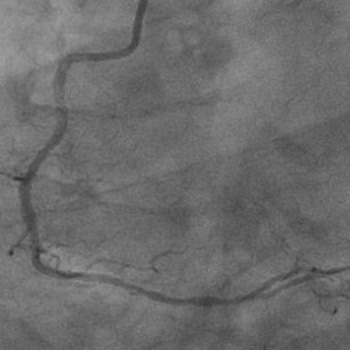 Procedure:
Procedure:
Following preloading with chewable 325mg of aspirin and 900mg of clopidogrel a 6Fr JL guiding catheter via the same radial sheath was used to engage the LCA and an All Star 0.014″ guidewire was put across the LAD stenosis that was sequentially predilated by a 2x10mm Elect balloon (Biotronik). 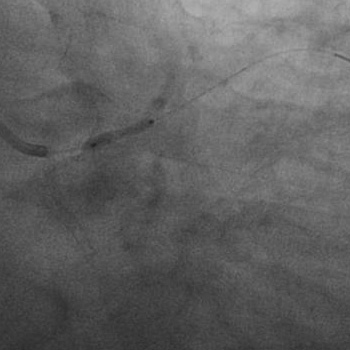 A 2.75x28mm Cypher Select stent
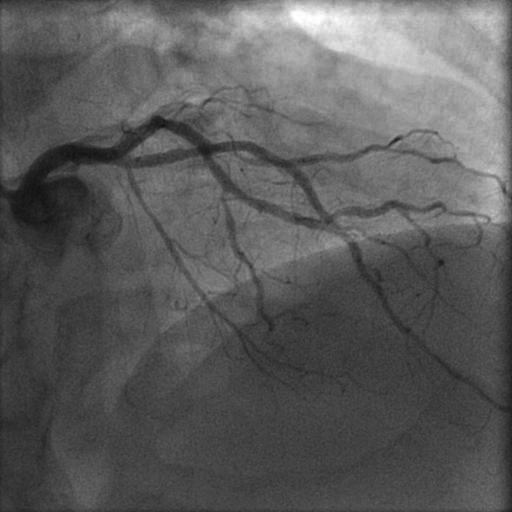
A 2.75x28mm Cypher Select stent  was deployed at 18atm to achieve TIMI 3 flow without dissection or residual stenosis.
was deployed at 18atm to achieve TIMI 3 flow without dissection or residual stenosis. The same guidewire was repositioned in the LCX artery; and the stenosis predilated with a 2×10 mm Elect balloon followed by implantation of a 3x10mm Cypher Select stent 16atm
The same guidewire was repositioned in the LCX artery; and the stenosis predilated with a 2×10 mm Elect balloon followed by implantation of a 3x10mm Cypher Select stent 16atm 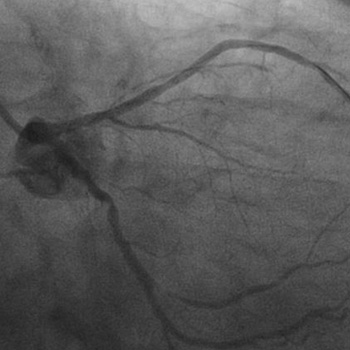 There was brisk antegrade flow with no residual stenosis or dissection.
There was brisk antegrade flow with no residual stenosis or dissection. 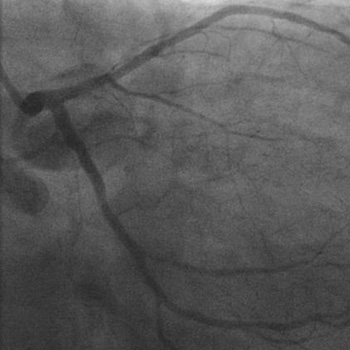
Conclusion:
TIMI 3 flow was achieved in both the LAD and LCX arteries without any residual stenosis nor any dissection. 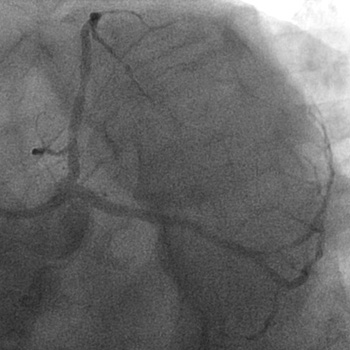
 The patient was maintained on injection eptifibatide. The patient’s pain and shortness of breath were relieved promptly subsequent to the PTCA/stenting of the LAD artery. He was discharged the next day on triple antiplatelet therapy consisting of 100mg of aspirin, 75mg of clopidogrel and 100mg of cilostazol twice a day.
The patient was maintained on injection eptifibatide. The patient’s pain and shortness of breath were relieved promptly subsequent to the PTCA/stenting of the LAD artery. He was discharged the next day on triple antiplatelet therapy consisting of 100mg of aspirin, 75mg of clopidogrel and 100mg of cilostazol twice a day.
Comments:
The severe intermittent chest pain accompanied by marked shortness of breath, elevated Troponin T levels, and significant ST segment elevation in the anterior precordial leads suggested an impending acute anterior MI. The tight proximal LAD stenosis with considerable visible thrombus burden indicated an on going myocardial infarction accompanied by a spontaneous thrombolysis/thrombogenesis. The presence of a large thrombus burden in the culprit vessel necessitated the administration of intracoronary bolus of eptifibatide. This case underscores the fact that the radial artery can be safely and effectively used in urgent complex interventions with minimal or no complications.
Conflict of Interest:
NIL