By Deepak Natarajan
Monday, June 30, 2008
Operator(s):
Deepak Natarajan(MD, DM) and Vivek Prakash(DM)
Affiliation:
Indraprastha Apollo Hospitals,New Delhi
Facility:
Departments of Cardiology, Indraprastha Apollo Hospitals, New Delhi, India
History:
A 69 yr old non diabetic male who had already received one bare metal stent each in his proximal LAD and mid RCA 4 years ago was readmitted for severe typical chest pain at rest, with ischemic ECG changes and positive troponin I values. On examination his heart rate was 60/min, blood pressure 180/110 mm Hg and he had a loud first sound with clearly audible S4. There was no evidence of heart failure.
Angiography:
His coronary angiogram revealed
Left main : normal.
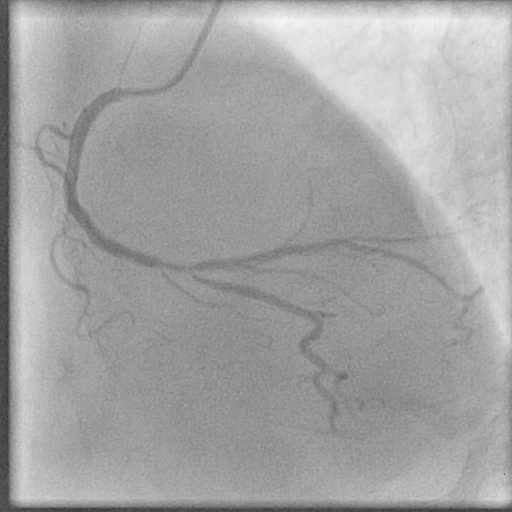
LAD : Patent stent and rest of the vessel normal (Figure 1).
Left Cx ; Patent stent with non critical proximal lesion of 30%.
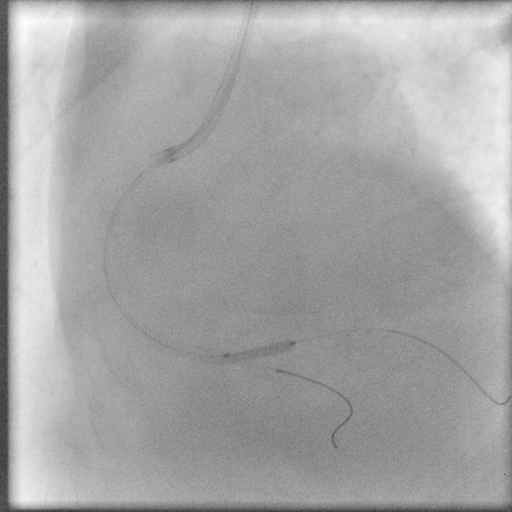
RCA ; Patent stent with 75 %to 90% stenosis involving the RCA/PDA bifurcation (Figure 2).
LV angiogram : Normal size LV with good LVEF of 60%.
{kind=link}
{kind=link}
Procedure:
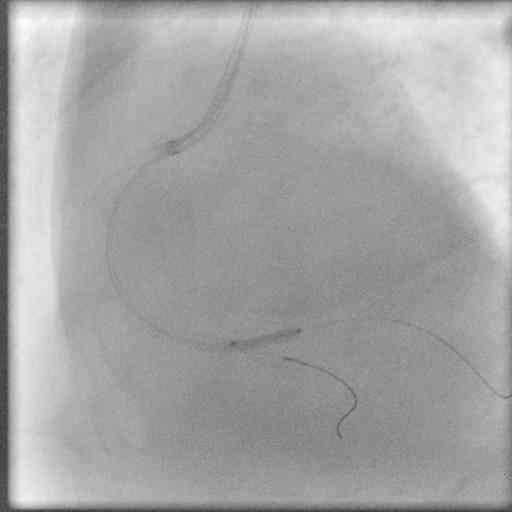
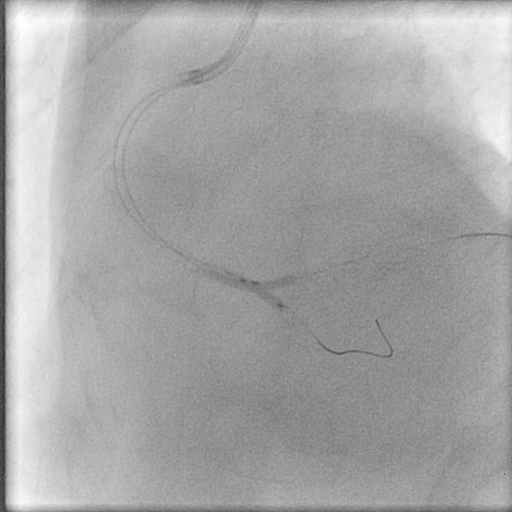
The right coronary artery was engaged with a 7Fr JR guiding catheter and a floppy wire 0.014 was introduced across the lesion into the PDA. Following predilatation by a 2.0/15 mm balloon a 2.5/20 PES was deployed at 18 atm (Figure 3). Angiograms demonstrated no residual stenosis in the stent but a 90% ostial stenosis in the Postero-lateral branch secondary to the stent (Figure 4). A new hydrophilic wire was negotiated across the stent into the large PLV branch and the struts dilated with an 1.5/10 mm balloon. A 2.0/10 PES positioned with its proximal end 2mm within the MV for an internal crush (Figure 5). Following deployment of the SB stent at 16 atm and a repeat angio the SB stent was next crushed with a 2.5+20 balloon at 20 atm (Figure 6 and Figure 7). The side branch stent struts were expanded by a 2+10 mm balloon at 16 atm (Figure 8) and eventually kissing balloon angioplasty was employed to achieve excellent results (Figure 9).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Conclusion:
There was no residual stenoses or dissection (Figure 10 and Figure 11). The procedure was preceded by 2 bolus injections of eptifibatide. He was discharged after 2 uneventful days in the hospital on aspirin,clopidogrel,cilostazol and fondaparinux.
{kind=link}
{kind=link}
Comments:
Management of bifurcation lesions continue to evolve rapidly with the provisional stenting approach considered to be the best. As the PLV branch had no lesion this was a classic case for provisional stenting of the side branch. The internal crush should prove to be the easiest,safest and most logical approach in such lesions.
Conflict of Interest:
None