In an international prospective cohort study more than 14,000 patients undergoing non cardiac surgery were studied ( Vascular Events in Noncardiac Surgery Patients Cohort Events Evaluation-VISION). There were 4802 patients who were using an ACE inhibitor or an angiotensin II receptor blocker who were 45 years or older. The researchers studied the ramifications of withholding the ACE inhibitor / ARB a day before surgery. Compared to patients who continued with the ACE inhibitor/ ARB , the 1245 (26%) patients who stopped the drugs 24 hours before surgery had lower adverse events. The composite of death, ischemia induced injury(assessed by troponin) or strike were less (125/1245;12%) was less than in those who continued (459/3557;12.9%). There was an absolute reduction of 0.9% and relative reduction of 18% (p <0.01). Post operative hypotension was similar in both groups ( Anesthesiology; October 2016).
ACE inhibitors and ARB’s are known to produce intraoperative hypotension but thus is the first time adverse clinical effects have been recorded. It is not clear as to why the 26% patients stopped ACE inhibitor/ARB prior to non cardiac surgery. There was significantly less intraoperative hypotension in those who did stop the drugs.
The Canadian Cardiovascular Society taking cognisance of the trial recommends stopping ACE inhibitor/ARB before non cardiac surgery. It is quite apparent that continuation of these medication does cause intraoperative hypotension and adverse clinical affects, but a randomized trial is required to replicate the conclusions of the VISION study.
The researchers concluded withholding angiotensin converting enzyme inhibitor or an angiotensin II receptor blockers before major noncardiac surgery was associated with lower risk of death and post operative vascular events.
Continued use of beta blockers for hypertension before major non cardiac surgery also raises risk of all cause mortality and major adverse cardiac events within 30 days of surgery,in a relatively low risk population. A Danish cohort study involving 55,000 patients reported increased mortality with continued use of beta blockers in low risk patients undergoing surgery . The AHA/ACC downgraded use of beta blockers from class I recommendation to IIb regarding beta blockers for high risk patients going in for noncardiac surgery. The European Society of Cardiology too downgraded recommendation to IIb.
The above trial had shown that men, those above 70 years of age, and patients undergoing emergency surgery were more susceptible to adverse effects of beta blockers. Patients receiving both a beta blocker and an ACE inhibitor also suffered greater MACE and mortality ( JAMA Intern Medicine 2015).
It would be prudent therefore to discontinue an ACE inhibitor/ ARB or beta blocker in a patient scheduled for noncardiac surgery, till randomised trials provide confirmation.

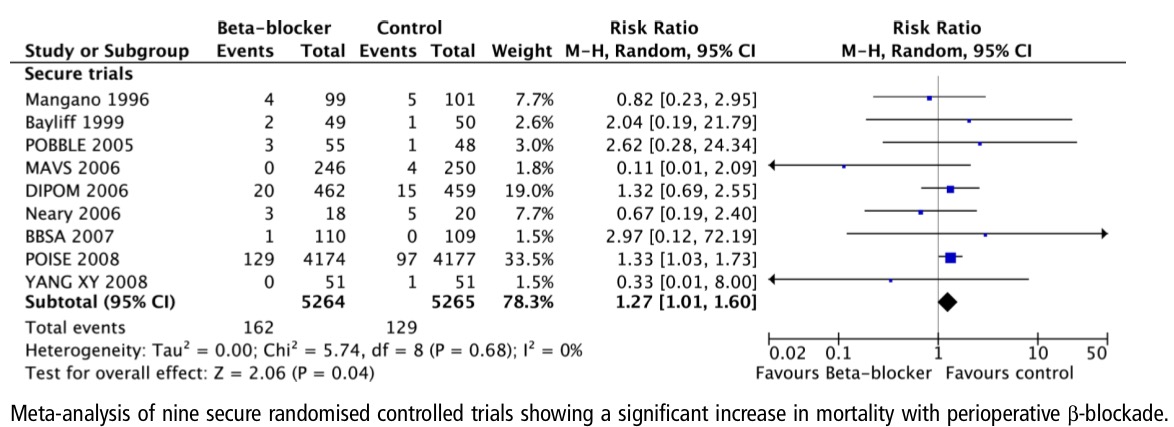
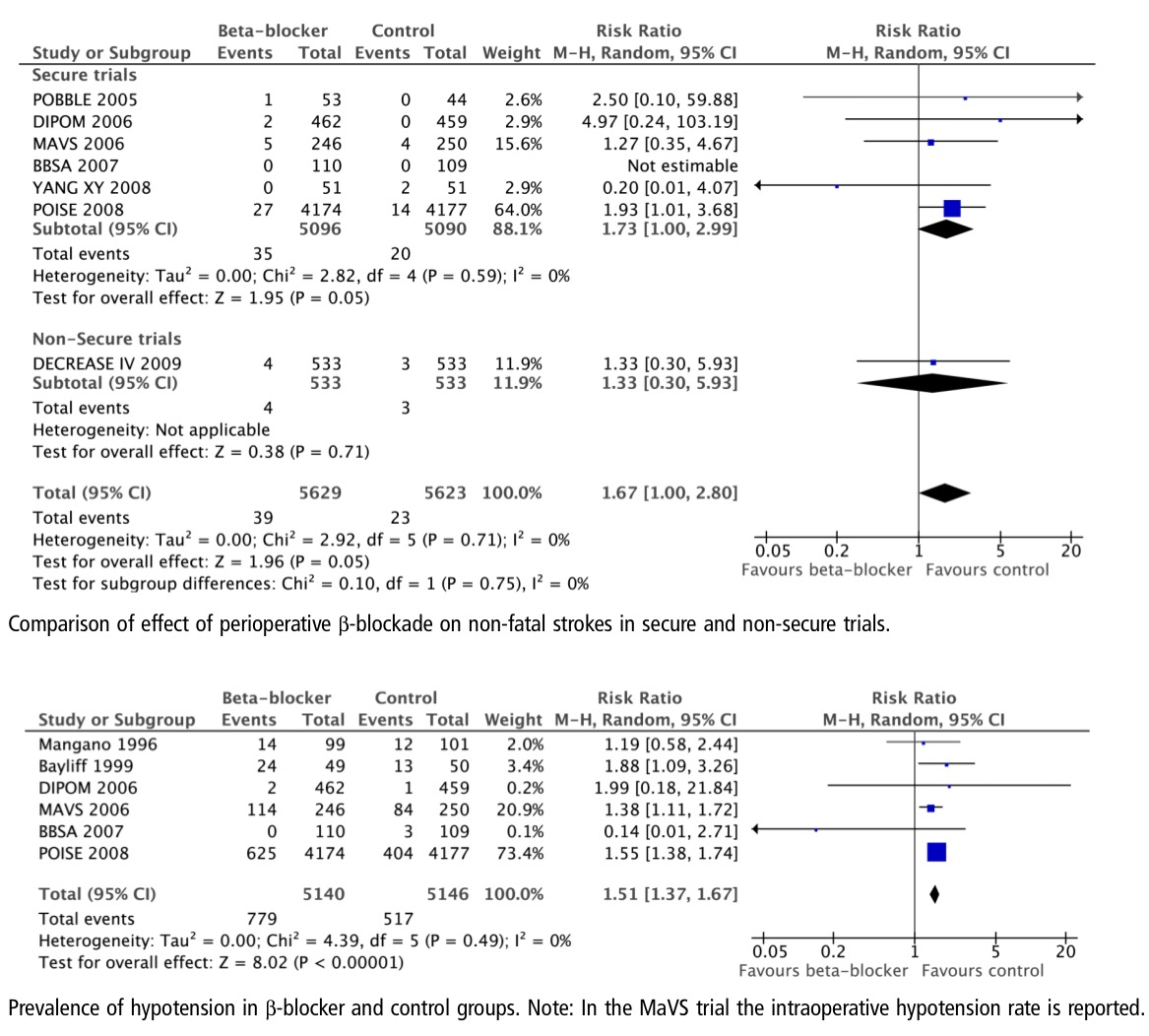
A rigorous meta meta analysis, including 9 randomized trials and involving more than 10,000 patients, concluded that peroperative treatment with a beta blocker during non cardiac surgery resulted in increased death by 27%. Beta blockers also increased stroke and hypotension. The implications for the cardiologist are enormous, the cardiologist can no longer advise a beta blocker as protection for non cardiac surgery in a patient with heart disease in the hope that the patient can be stented subsequent to surgery. The data available suggests otherwise, the beta blocker could actually kill the patient during surgery (Heart;31st July 2013).