By Deepak Natarajan
Monday, February 09, 2009
Operator(s):
Deepak Natarajan, MD, DM and Sandeep Vohra, MD
Affiliation:
Indraprastha Apollo Hospitals,New Delhi
Facility:
Departments of Cardiology and Radiology
Indraprastha Apollo Hospitals, New Delhi, India
History:
A 65 year old hypertensive patient was admitted for Troponin T negative unstable angina. He was having retrosternal chest pain for the previous 5 days with radiation to left arm at rest and during exercise accompanied by perspiration. His ECG showed ST segment depression in the chest leads.
Angiography:
- LM was normal.
- LAD was normal
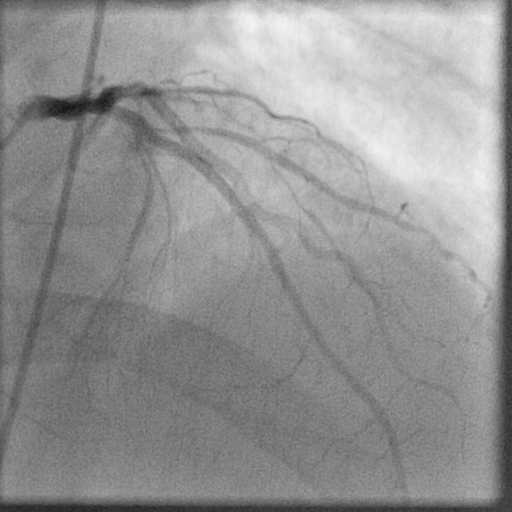
 The second diagonal branch (D2) was large with an 80% ostial stenosis extending to proximal segment of the vessel.
The second diagonal branch (D2) was large with an 80% ostial stenosis extending to proximal segment of the vessel. - LCX was normal
- RCA was aberrant and arising from the opposite left sinus of Valsalva (ARCAOS) with an 80% mid-segment stenosis.
 The ARCAOS was hooked using a 6Fr multipurpose diagnostic catheter.
The ARCAOS was hooked using a 6Fr multipurpose diagnostic catheter.
Procedure:
Two bolus injections of eptifibatide were administered I/V before the PCI procedures. The ARCAOS was intubated with a 6Fr JL guiding catheter, and a 0.014″ BMW guidewire was placed across the stenosis followed by direct stenting with a 2.5x15mm Taxcore paclitaxel-eluting stent at 16atm 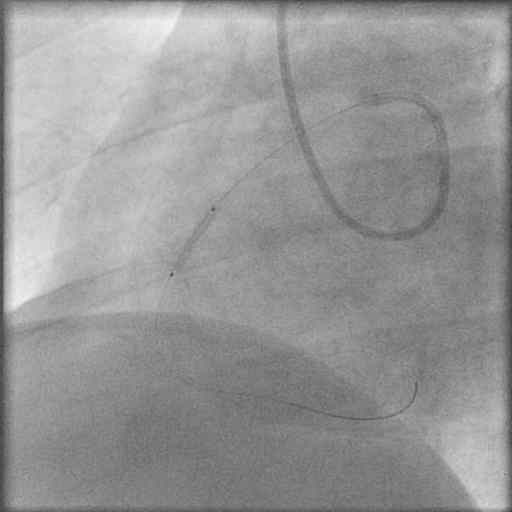 Brisk antegrade flow was achieved with no dissection or residual stenosis.
Brisk antegrade flow was achieved with no dissection or residual stenosis. 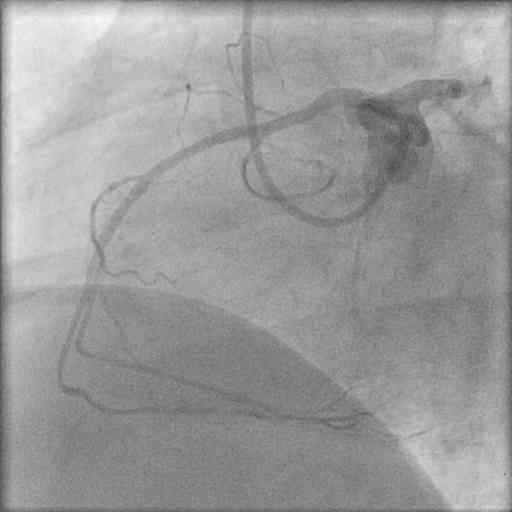
The left coronary artery was engaged with a 7Fr JL guiding catheter, and two floppy guidewires were positioned in LAD and D2. The D2 lesion was predilated with a 2x10mm Elect balloon, and a 2.5x12mm PRO-kinetic cobalt chromium was deployed at 14atm. 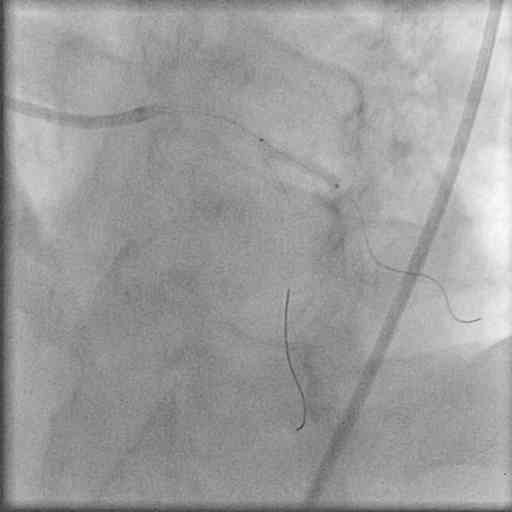 The procedure was completed with kissing balloon inflations
The procedure was completed with kissing balloon inflations  that ensured TIMI 3 flow without any residual stenosis or dissection.
that ensured TIMI 3 flow without any residual stenosis or dissection. 

Conclusion:
A 64- slice computerized tomography coronary angiogram (CTCA) confirmed the dominant right coronary artery arising from the left sinus of Valsava with a patent stent in the mid segment. Moreover, the ARCAOS was coursing between the aorta and pulmonary artery. 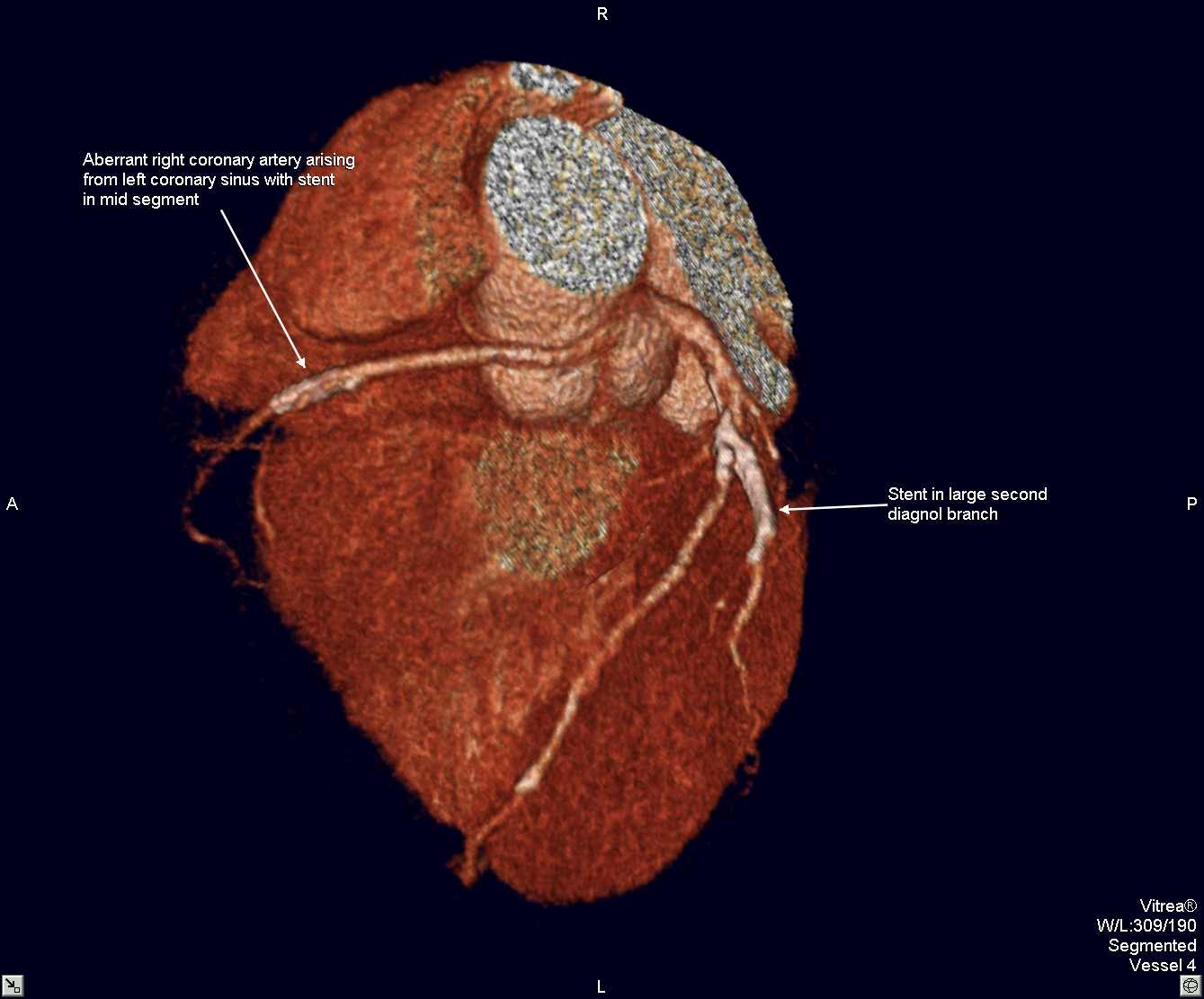
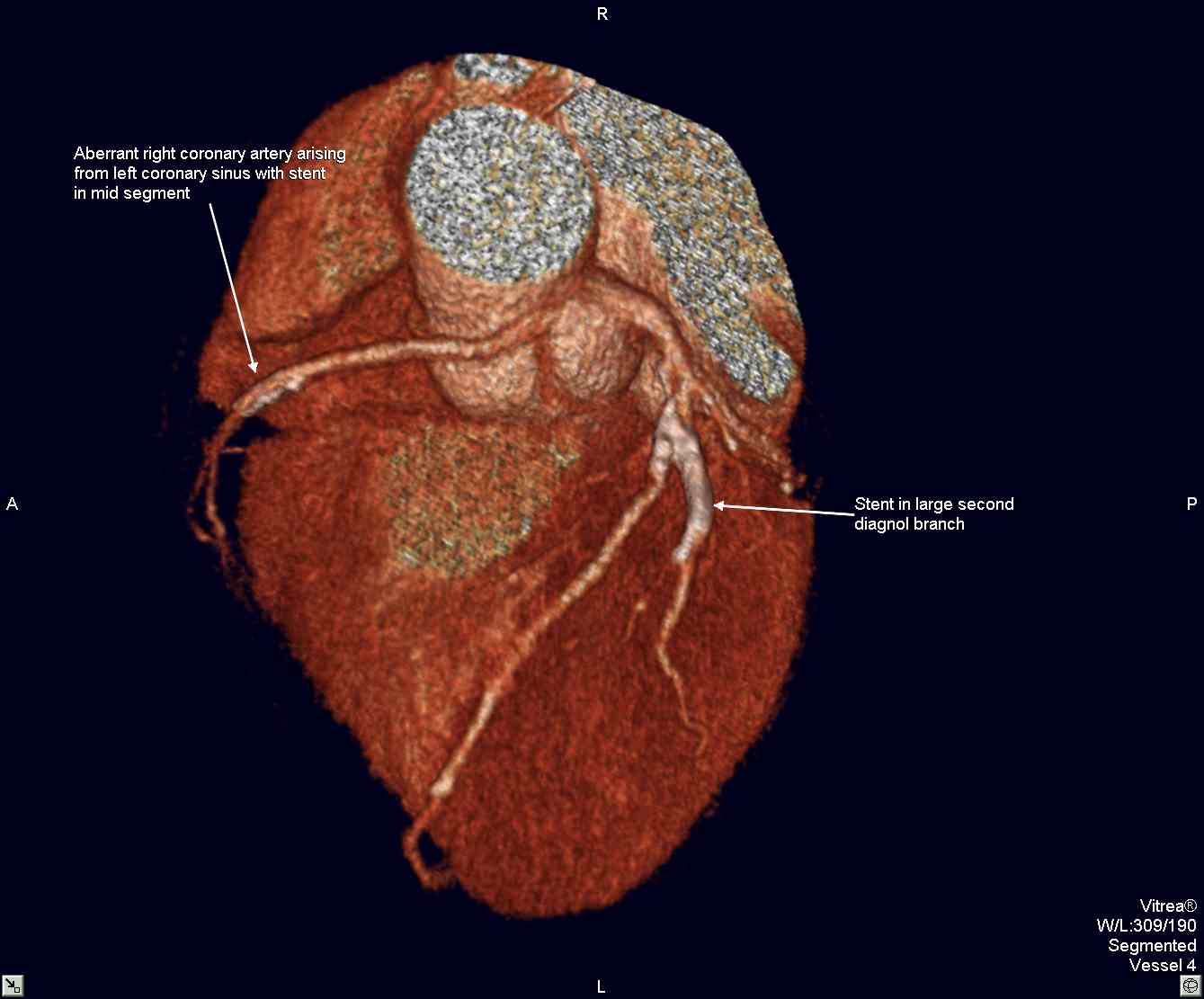
 The stent in D2 was also patent.
The stent in D2 was also patent.
Comments:
The exact pathophysiology resulting in life threatening cardiac ischemia continues to evolve albeit it is established that ARCAOS may result in sudden cardiac death. The incidence of coronary anomalies may be 5% and that of ARCAOS alone may as high as 1%. There is currently no formal protocol for screening aberrant coronary arteries in athletes and soldiers. Besides the scissoring effect of the great vessels on an ARCAOS producing significant ischemia, it has also been demonstrated that the initial portion of an ARCAOS can be compromised as it travels within the intramural aortic wall. This can best be determined by IVUS, and there is a report of PCI with stenting of the most proximal intramural part of an ARCAOS causing cardiac ishemic symptoms. This case demonstrates that in a symptomatic middle aged male with ARCAOS the cause of ischemia can be atherosclerosis and which may be easily managed by PCI.
Conflict of Interest:
NIL