By Deepak Natarajan
Monday, July 28, 2008
Operator(s):
Deepak Natarajan, Vivek Prakash and Jasbir Singh
Affiliation:
Indraprastha Apollo Hospitals,New Delhi
Facility:
Department of Cardiology, Indraprastha Apollo Hospitals, New Delhi, India
History:
A 59 year old man was admitted for severe resting chest pain over last 2 weeks. Past medical history was significant for hypertension and heavy smoker for more than two decades. His baseline ECG revealed non specific ST-T wave changes accompanied with increase in serum troponin I levels. There was no family history of heart disease.
Angiography:
- LM: 95% distal Left main
- LAD: 95% Ostial stenosis extending from the distal LM. 85% proximal LAD stenosis
- LCX: Large calibrre with mo significant stenosis.


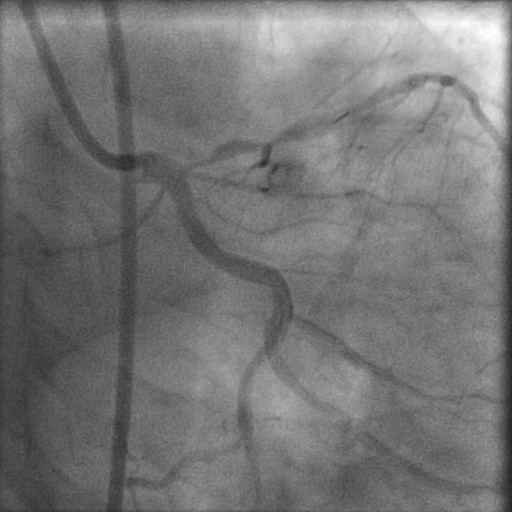
- RCA: Luminal irregularities in mid segment.
- LV: Ejection fraction of around 55%.
Procedure:
Subsequent to informed consent to PCI the left coronary artery was engaged by a 7F JL 3.5 guiding catheter and a 0.014″ floppy wire was advanced into the LAD across the lesions. Both lesions (distal LM to ostial LAD and the proximal LAD) were sequentially pre-dilated with 1.5×15 and 2×15 mm balloons 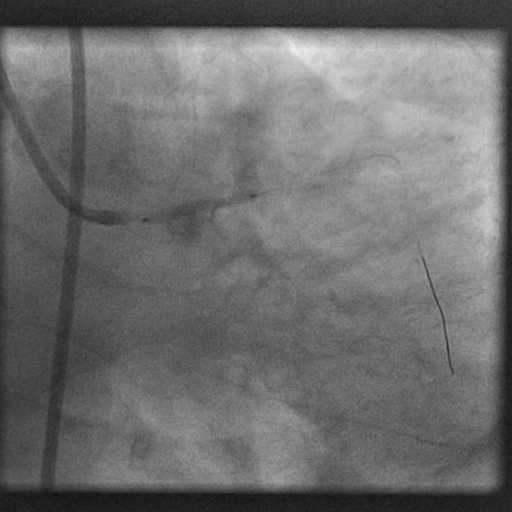 up to 14 atm. Following pre-dilatation a 3×32 mm paclitaxel eluting stent was placed from the most distal part possible of the LM artery into the LAD to cover the left main and both ostium and LAD proximal stenosis. This was deployed up to 20 atm.
up to 14 atm. Following pre-dilatation a 3×32 mm paclitaxel eluting stent was placed from the most distal part possible of the LM artery into the LAD to cover the left main and both ostium and LAD proximal stenosis. This was deployed up to 20 atm. 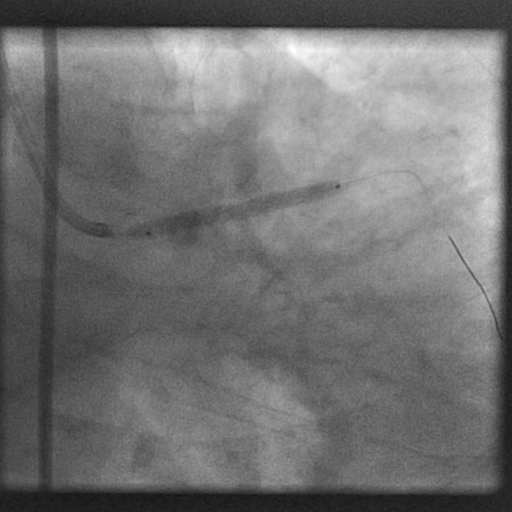 Additional postdialtation was performed with a 3.5×10 mm high pressure balloon up to 24 atm.
Additional postdialtation was performed with a 3.5×10 mm high pressure balloon up to 24 atm. 
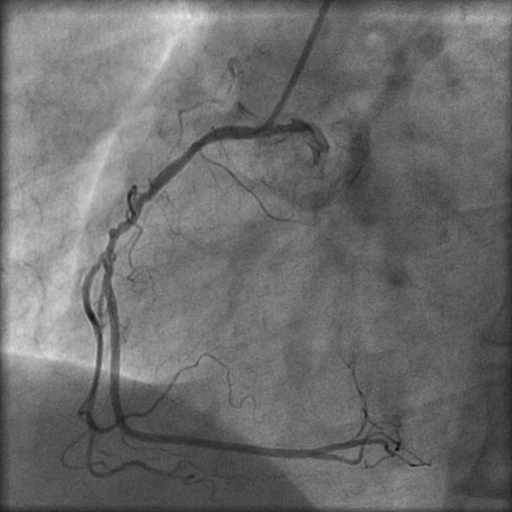
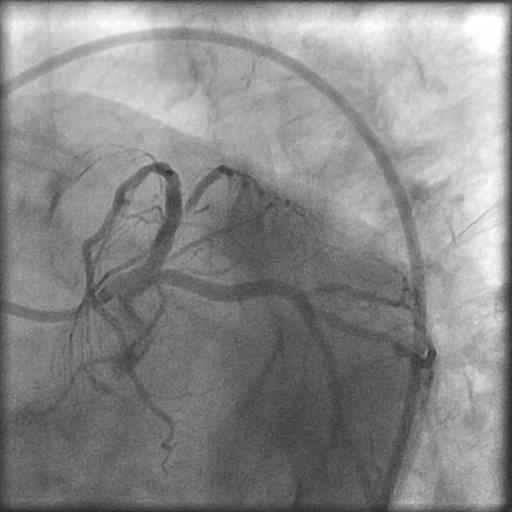
 The final angiogram showed a fully expanded stent without residual stenosis or dissection. There was no compromise of the LCX artery.
The final angiogram showed a fully expanded stent without residual stenosis or dissection. There was no compromise of the LCX artery. 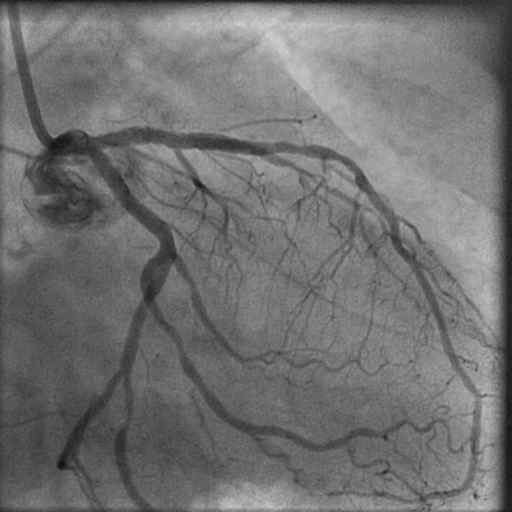
Conclusion:
Cross over stenting is the simplest technique to employ in distal LM lesions not involving the left circumflex artery. In this case TIMI 3 flow was achieved with no complications.
Comments:
In this case the choice of cross over stenting was simple because there was no lesion in the circumflex artery. The approach for distal LM bifurcation not involving the left circumflex or a small / insignificant circumflex artery is cross over stenting from the LM to the LAD artery. In the event of jailing or compromise of the left circumflex post cross over stenting the situation should be dealt accordingly, usually with balloon angioplasty or another stent. The distal LM artery though involved was stenosed at its most distal tip adjacent to the LAD ostium. The procedure was quick and uncomplicated. The patient was discharged a day after procedure on triple antiplatelet therapy for the next one month and 2 days of injection fondaparinux.
Conflict of Interest:
None