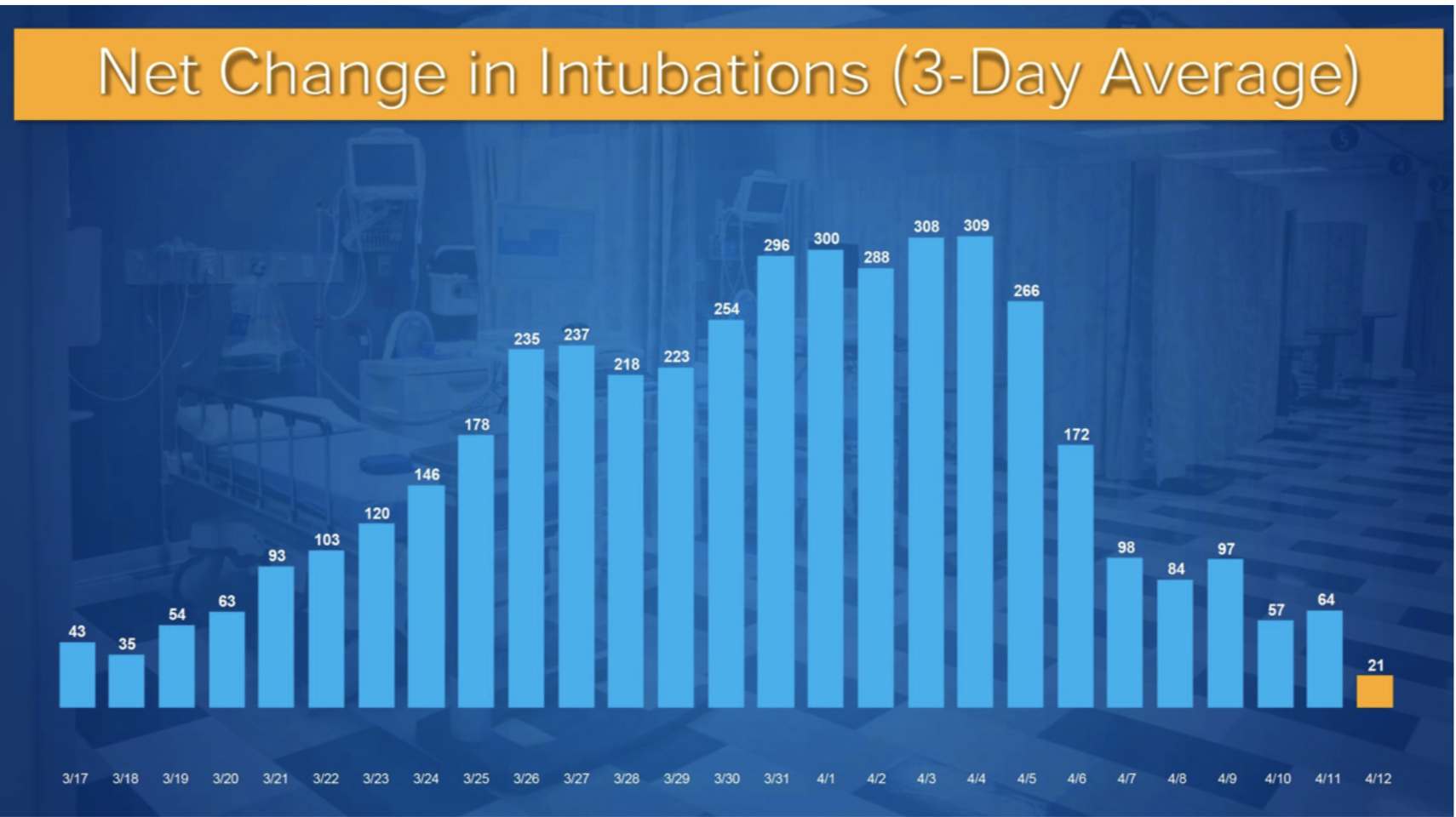

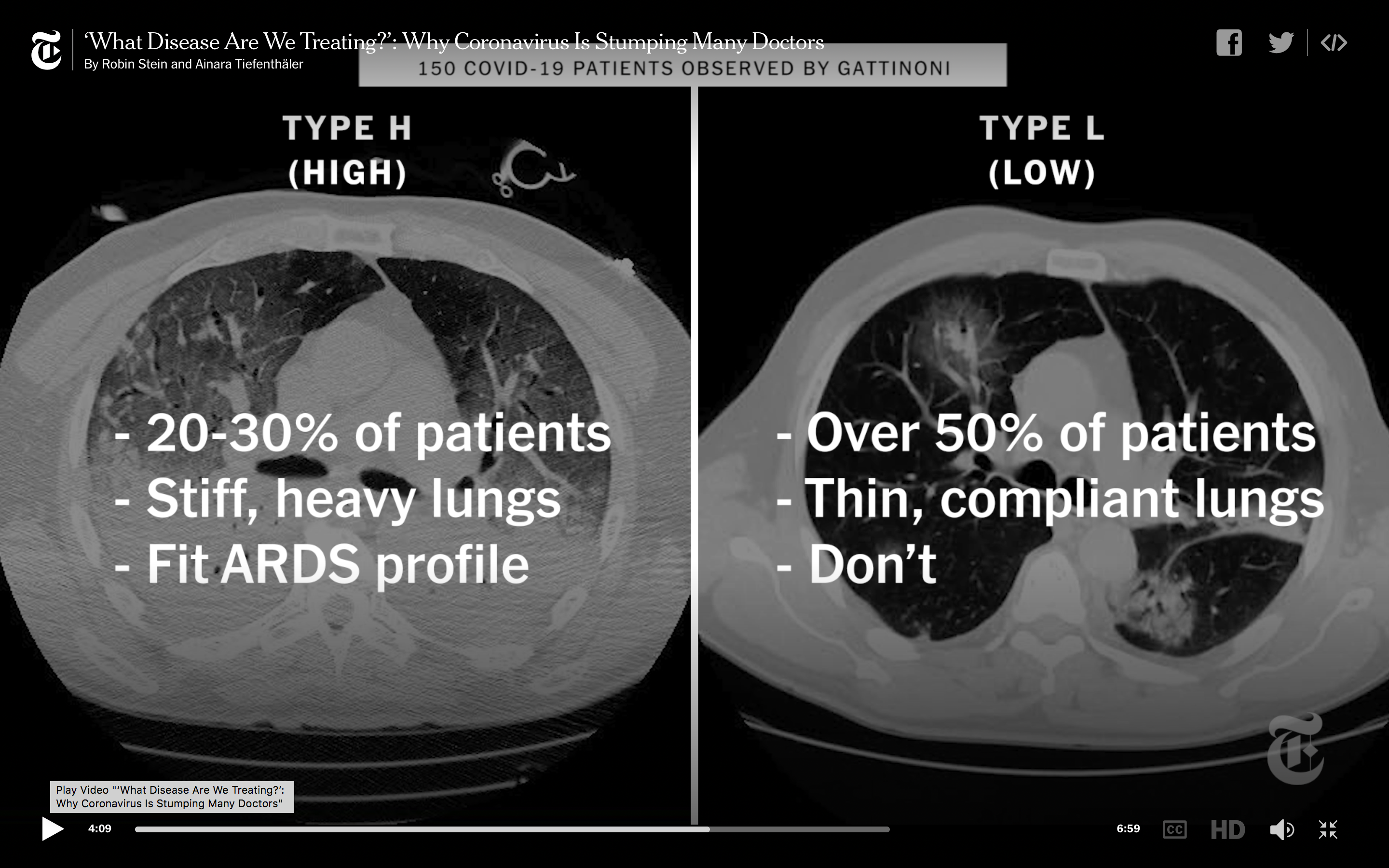
Each day brings more information of the SARS-CoV-2, of its infectivity, its lethality, pathogenies and treatment. One of the most striking revelations has been that patients put on ventilators do extremely badly. Just about every centre reports very high rates of death once a tube is put in a patient. Some critical care doctors have stuck out their necks to explain that lung pathology in Covid-19 patients seems different from that of acute respiratory distress syndrome (ARDS). Professor Gattinoni, a leading expert from Italy, has suggested that the lungs of most Cover -19 patients retain their mechanical capacity to function despite severe hypoxia. Clinicians in New York have begun to notice that patients with Covid-19 having low oxygen saturations continue to lucid and clear. It is not uncommon to find a patient with an oxygen saturation as low as 50% speaking on the phone. The term “happy hypoxia” has been given to the condition, only for these patients to suddenly collapse. The initial paradigm of incubating patients as soon as oxygen saturation begins to drop is drawing sceptics. It is slowly being realised that patients with Covid-19 have a unique lung disease, not the classical ARDS. Treating doctor shave realised that somehow intubated patients fare badly, with mortality ranging from 30 to almost 100%. One explanation discussed among critical doctors is that air pushed in at high pressure by ventilators may be causing more harm to lungs than providing relief to them. It has been noticed by some doctors , serendipitously, that a patient with severe hypoxia but conscious did better with oxygen provided by a tube in the nostril. One trick employed is to turn the patient to her left or right or even prone (on the tummy). There is dramatic improved in oxygen saturation within minutes of applying this simple technique. Most probably the prime minister of England was treated with simple oxygen delivery. At the most he may have been given oxygen by continuous positive airway pressure or CPAP. The Covid-19 lugs seem to be more like those of high altitude sickness. As a New York doctor explains it is like dropping some on on the peak of the Mount Everest without any time to acclimatise. The SARS-Covid-19 virus, unlike conventional pneumonia, attacks both lungs. The patients come to hospital with low oxygen levels but not in distress. The usual patient is in acute distress once oxygen drops below 80%, but not the Covid -19 patient. The Covid-19 patient has a strange slime in his airsick that prevents oxygen exchange in the lungs. Increasing the force with which the ventilator can pump in air is of little or no help. Maybe ventilators may work at lower pressures in selected patients, but this will need a randomised trial. For now many critical care specialists are batting for simple oxygen administration to the patient, while she is kept in a prone position. No wonder there has been a substantial reduction in use of ventilators in Covid-19 patients in New York city. The current mantra is to use ventilators in selected cases but used to push in oxygen less aggressively.
The simple oxygen administration technique is buttressed by the first autopsy report form one of the top US hospitals. The report consists of only 2 patients , but is revealing all the same. The first patient who died from the virus was an obese 77 years old hypertensive man, whose autopsy showed that the lung sacs were smeared with a substance that resembled thick paint. The man was confirmed to be positive by RT-PCR. The man had been symptomatic for 6 days, he had fever and chills. He died before he could be put on a ventilator. The lung sacs were inflamed and damaged, and full of lymphocytes ( proof of damage due to virus).
The second case albeit infected by SARS-CoV-2 did not die from it. The 42 years old man did not have the slime in his air sacs, he died of bacterial pneumonia. This man was admitted in a critical condition to hospital for fever, cough and shortness of breath. A CT scan done before he died showed bilateral ground glass opacities as well as bilateral pneumonia. Nasopharyngeal swabs were positive for SARS-CoV-2 by RT-PCR, but both lung swabs were negative. A standard respiratory pathogen was also negative. Bacterial cultures grew Escherichia coli and Proteus mirabilus. Under the microscope it was seen that the lungs had bronchopneumonia and aspirated food particles. The man had suffered from a muscular weakness disease. The final autopsy listed Covid-19 as a condition but not the cause., the manner of death was listed as natural. The patient had most probably died of bacterial pneumonia likely caused by aspiration. The authors of the paper emphasise “Therefore, this patient likely died with COVID-19, not from COVID- 19. These cases illustrate the challenges that pathologists and the medical community at large will face in deter- mining the cause of death in decedents who test positive for SARS-CoV-2. Some findings will represent true virus- related pathology, while others will reflect superimposed processes or unrelated illnesses.” Greater experience as the pandemic unfolds will help forensic pathologists tease out cases that die from SARS-CoV-2 rather than perishing with it.
It has been difficult explaining the difference between a patient dying from SARS-CoV-2 as compared to some one dying from some other disease but simultaneously infected by this virus. A postmortem is the only method for confirmation albeit even this could be demanding; but clinical confirmation of cause of death will certainly prove to be perplexing in a lot of cases. It is for this reason that I am unsure of the numbers of Coivid-19 deaths being provided by most countries. The Italians too have conceded that they are not sure of the exact number of deaths caused by SARS-CoV-2. Moreover the CDC is quite flexible regarding mention of cause of death; even confirmation of the presence of SARS-CoV-2 is not mandatory while filling death certificates.
The Times (London) has reported yesterday what I consider the only bright news in the previous 3 months regarding the Covid-19 pandemic. This information is considered a “leak.” Apparently a video is floating around that reveals a University of Chicago reviewing results for her colleagues, on a broad spectrum anti viral medicine called remdesivir. The university had recruited 125 patients with Covid-19 into 2 trials, one trial included 113 severe patients. There was no control or placebo arm, all patients were treated with intravenous remdesivir. Fever got reduced in many patients, some were taken off ventilators within a day and most patients did not need the full 10 days course with remdesivir. Importantly only 2 patients have died.Most patients were leaving hospital as early as 6 days. This is remarkable news if true. One hopes the leak was not deliberately engineered by the manufacturing company. In a statement, the University of Chicago said “drawing any conclusions at this point is premature and scientifically unsound.”The news item fails to inform us of the seriousness of the illness in the recruited patients, at what point of time the drug was administered, or how many were on ventilators . Moreover the trial is yet to be published, the company however has recruited 2400 severe Covid-19 patients from 152 clinical trial sites all over the world. More than 1600 patients with mild symptoms have also been included in clinical trials from across the world.
DOI: 10.1056/NEJMoa2007016
A small trial with remdesivir was published recently that included 53 patients with severe Covid-19 patients. All patients had oxygen saturation less than 94%, with almost half needing ventilators and 4 patients were on ECMO machine. All patients received remdesivir for 10 days on compassionate use basis. Improvement was seen in more then two thirds of patients , with 17 of 30 patients on mechanical ventilation getting off the machine. Almost half of patients studied became fit enough to be discharged. Mortality was 5% (1m of 9) in those not needing ventilation and 18% (6 of 34) in those attached to a ventilator. This was not a randomised trial, and did not have a placebo group. The trial should be considered preliminary with a hint that remdisivir may be effective in severe patients with Covid-19. Data form the larger trials will provide much needed clarity on treating the SARS-Cov-2 induced pandemic. Till then all reports should be considered anecdotal, even if there are some case reports showing marked improvement.
How does the drug work ? Remdesivir does not attack the virus directly. It instead goes after the copying machine of SARS-CoV-2.These viruses have a genome that consists of a strand of RNA. To make copies of themselves, they rely on a molecule called a polymerase to string together the individual building blocks of the viral genome. Remdesivir mimics the appearance of one of the RNA letters, adenosine. It looks so similar that the polymerase can unknowingly pick it up instead of the real adenosine and insert it into the strand of viral genome that’s being constructed. Once in place, the analog acts as a cap, preventing any additional pieces from being strung on. This leaves the strand short of the full genome. The virus can’t go on to replicate or infect other cells.As a researcher put it “The polymerase grabs it almost accidentally and uses it in place of adenosine.”The usual caveats apply, the trials done so far have not included controls, so a bias can never be ruled out. A randomised trial is scheduled by the NIH (US), and we will have to wait for the results before drawing any conclusions.
The good news is that inspite of increased testing the number of new cases are in the decline, and number of deaths too follow the same trend. The WHO has reported a total of 437 deaths yesterday with 23 new deaths . Coronavirus cases in India rose to 14,792 on Saturday evening, according to the health ministry website. The death toll in the country stood at 488. 75.3% of those who died were over 60 years old. In 83% of the deaths, the patients had co-morbidities like diabetes, hypertension and heart disease. One should expect further reduction both in number of fresh cases and deaths with increase in temperature.