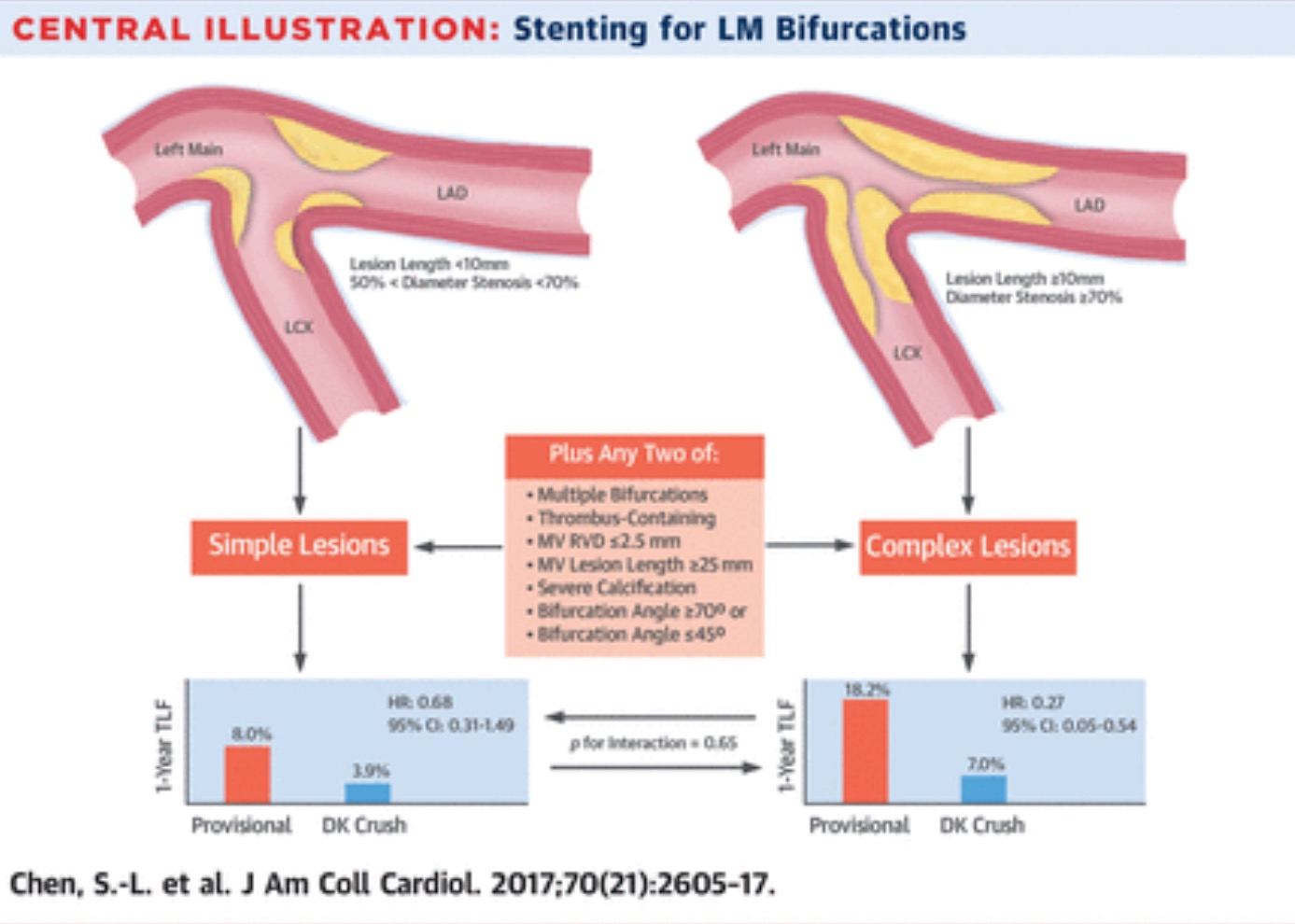
Provisional stenting (PS) is the most common technique employed in unprotected distal left main disease bifurcation lesion when patients undergo percutaneous coronary intervention (PCI). The double kissing (DK) 2 stent technique has been found to effective for non left main bifurcation lesions. Recently JACC published a paper that reports the DK technique for kept main lesions. Thus study randomised patients with distal left main bifurcation lesions to the DK technique and PS. The researchers randomised mire than 480 left main bifurcation patients to DS and PS technique. The primary outcome of death, target vessel myocardial infarction and target vessel revascularisation occurred in significantly less in DK technique as compared to PS; 5% versus 11%; p=0.02. DK technique also resulted in lesser myocardial infarction alone with fewer stent thrombosis. Clinically driven target lesion failure and restenosis were also significantly less with the DK technique. There was however no significant difference in cardiac death in the two cohorts. Crucially in complex left main lesions ( more than 10 mm in length and greater than 79% stenosis, the DK technique reduced target vessel failure significantly from 18% to only 7%. In simple lesions target lesion failure was reduced from 8% to 2%. The researchers concluded that in true distal left main bifurcation lesions DK 2 stent technique resulted in significantly less target lesion failure at the end of one year than the provisional stenting strategy. This is the first randomised trial comparing DK crush with provisional stenting in left main bifurcation lesions. The number needed to prevent target lesion failure was 20 overall, and only 9 in complex lesions.
Currently PCI has established itself as a viable and safe alternative to CABG in patients of true distal unprotected lesions. Provisional stenting is the preferred technique because of simplicity and reasonable efficacy in non left main bifurcation lesions. Provisional stenting mandates stenting the side branch only if there is no or minimal flow in the side branch after stenting the main branch, regardless of “jailing” the side branch. T stenting is done when the side branch originates at an angle of 70-90 degrees from the main branch. If the angle is less than 70 degrees the Cuolette or DK crush is recommended. The DKCRUSH-V trial mentioned above documents significant reduction in stent thrombosis, which may be considered as a ‘hard’ endpoint because it is associated with mortality. The editorial to the JACC article points out that both EXCEL and NOBLE trials (both used provisional stenting) may have recorded superior results in the PCI arm as compared to CABG, had DK crush technique be used.
The EXCEL trial ( NEJM October 2016) had concluded that PCI with sirolimus eluding stents was non inferior to CABG surgery in patients of left main disease with low or intermediate SYNTAX scores over a period of 3 years, with respect to the composite end point of death, myocardial infarction or stroke. EXCEL had randomised 1905 patients of left main disease with low or intermediate SYNTAX complexity to PCI or CABG surgery and followed the patients for 3 years. The EXCEL trial had defined significant left main disease as a lesion greater than 70% or if between 50% and 70% to be accompanied by an FFR of less than 0.80 or minimal luminal area of less than 6 mm square by IVUS.

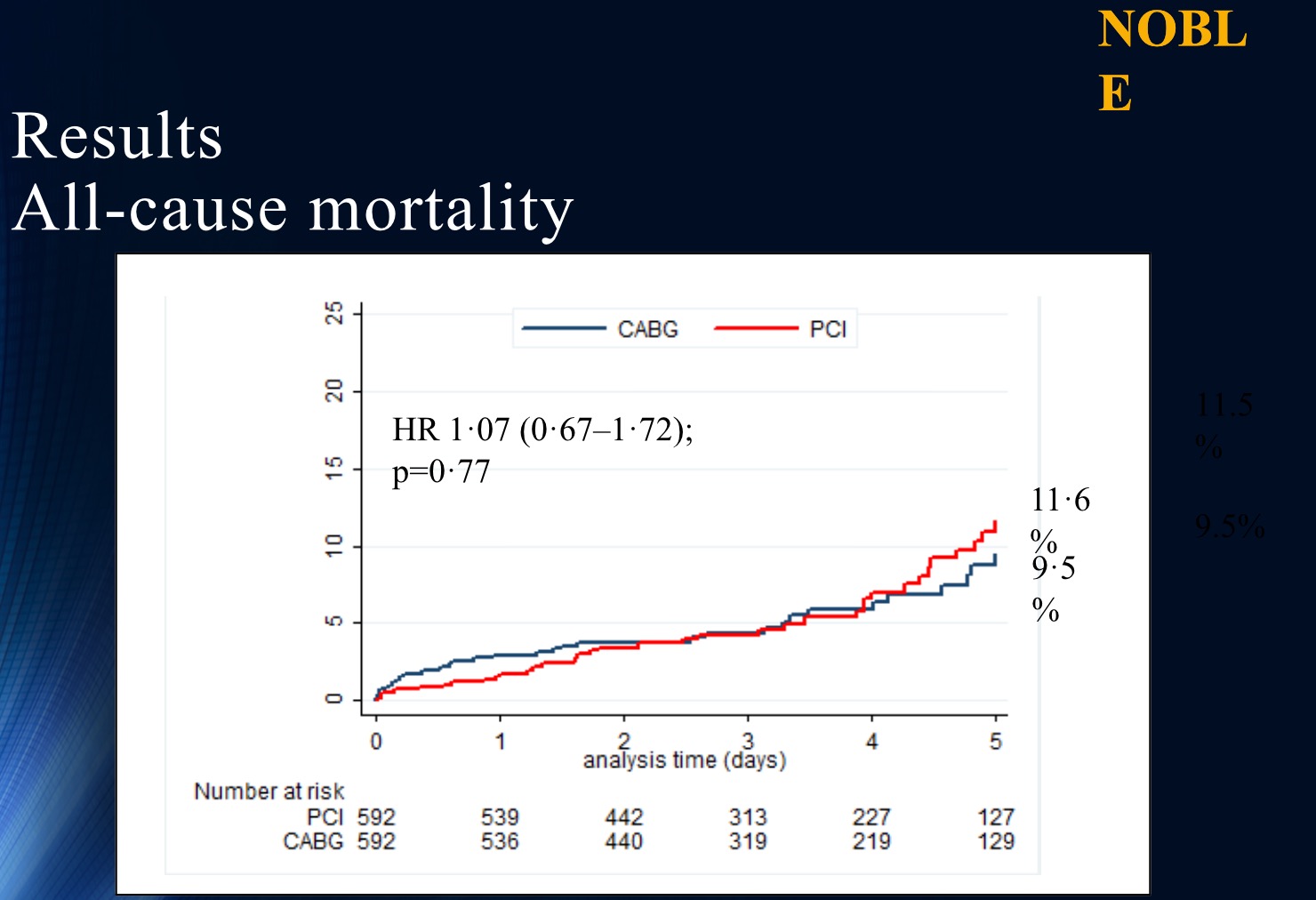
The NOBLE trial on the other hand randomised 1200 patients of left main disease to PCI with a biolimus eluding stent or CABG surgery. The lesion had to be greater than 50% on visual assessment or have an FFR ratio less than 0.80. Current international guidelines recommend CABG or PCI ( level of recommendation I B) for left main lesions of low complexity ( SYNTAX score less than 23) ; and also lesions of intermediate complexity ( SYNTAX score of 23 to 32) with 2A as level of recommendation for PCI. The average SYNTAX score in the NOBLE trial was 22.5 with 80% being distal bifurcation lesions. Preevaluation with IVUS was done in 47% of patients and 74% of patients had post evaluation with IVUS in the NOBLE trial. There was no difference in mortality but significantly greater non procedural myocardial infarction and repeat revascularisation with PCI as compared to CABG. PCI did not meet non inferiority at 5 years for MACCE as compared to CABG.
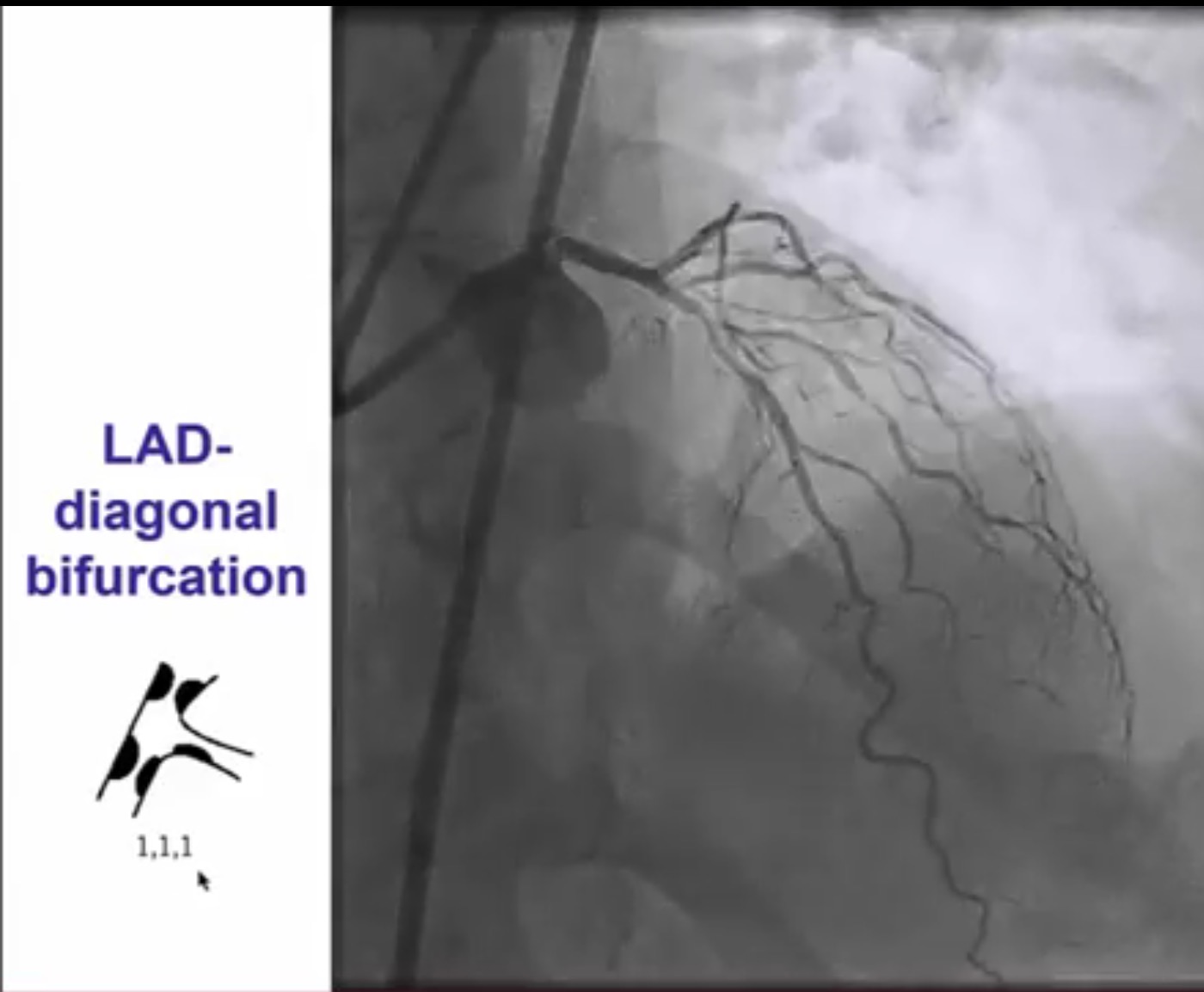
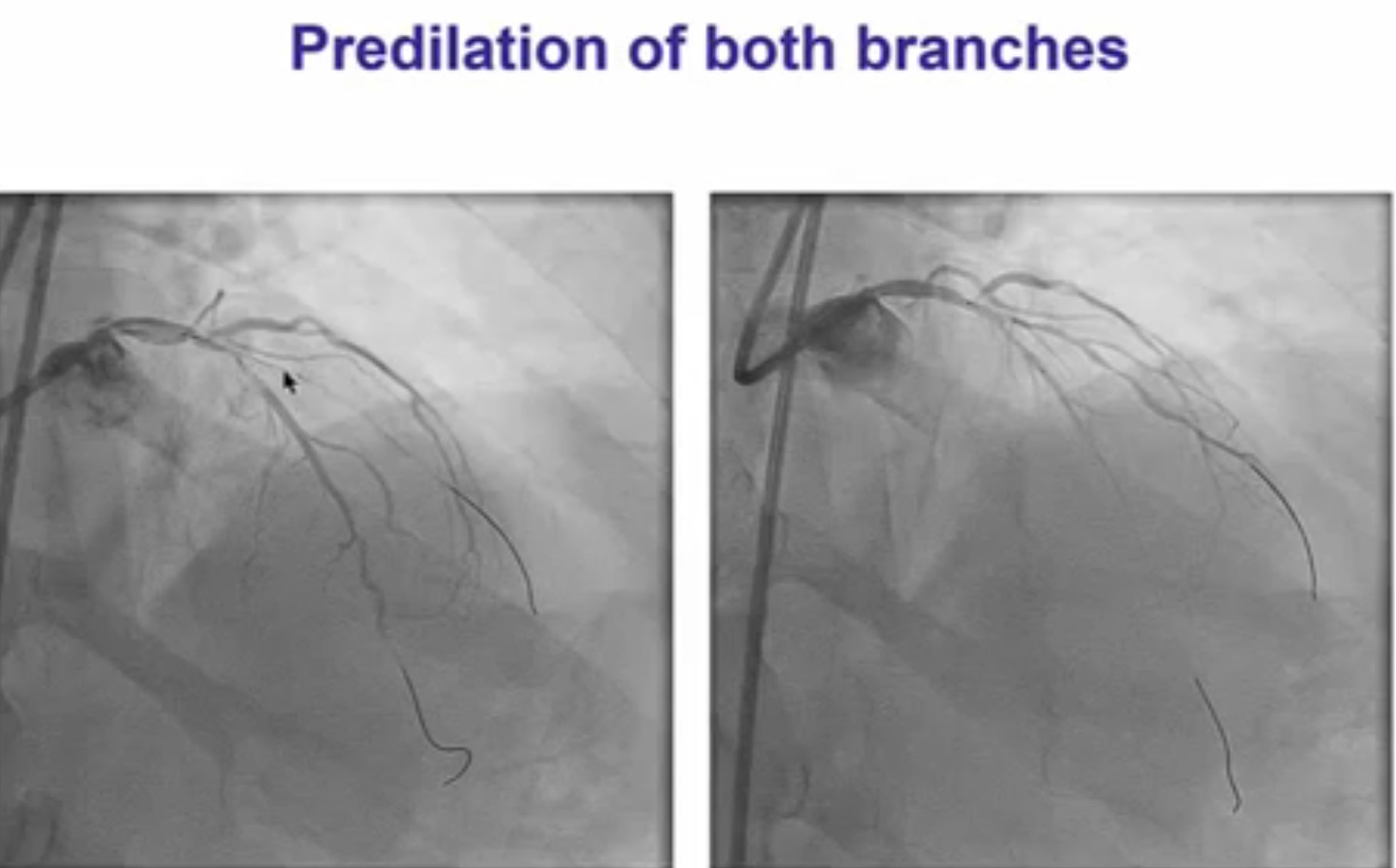
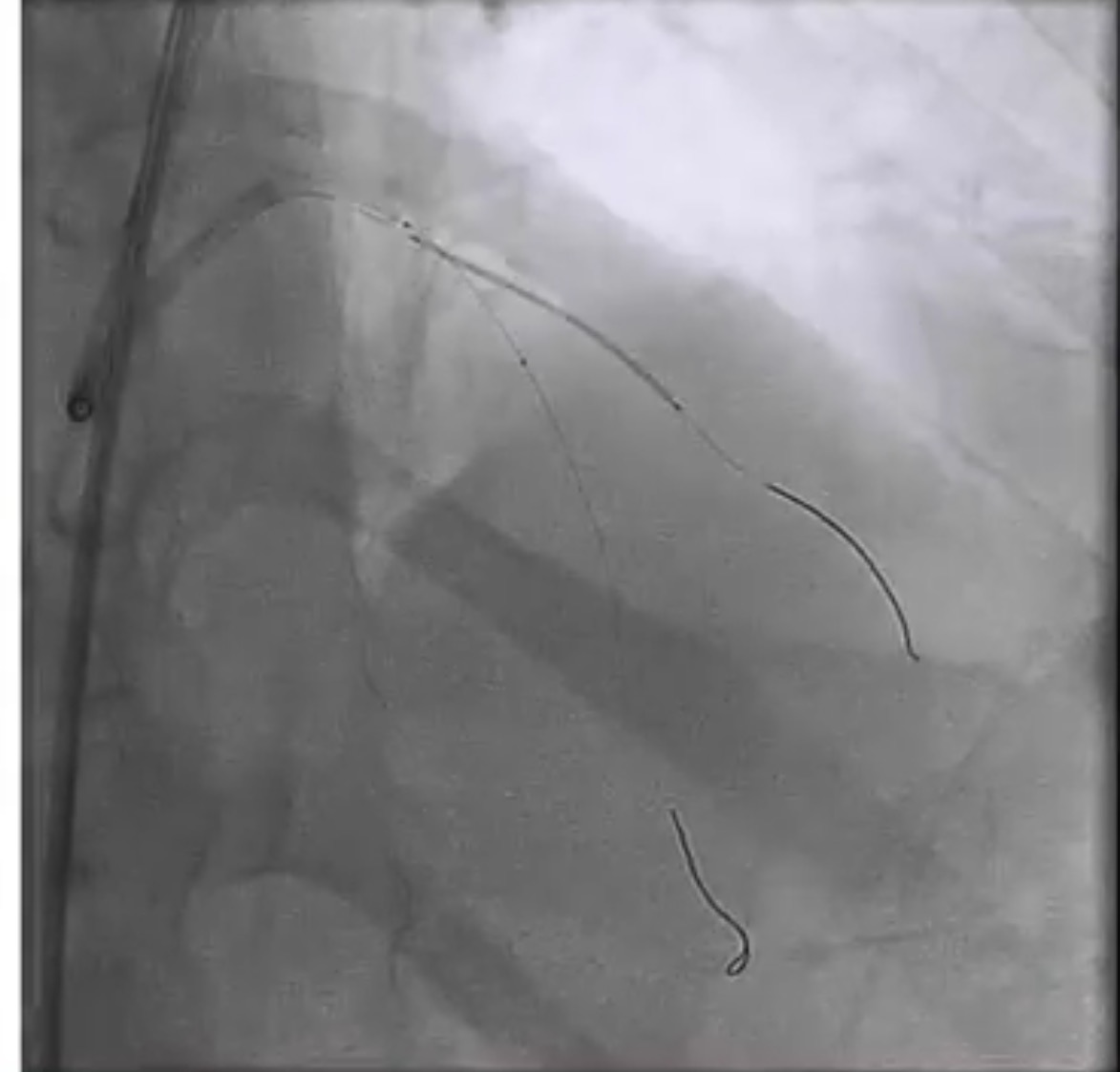
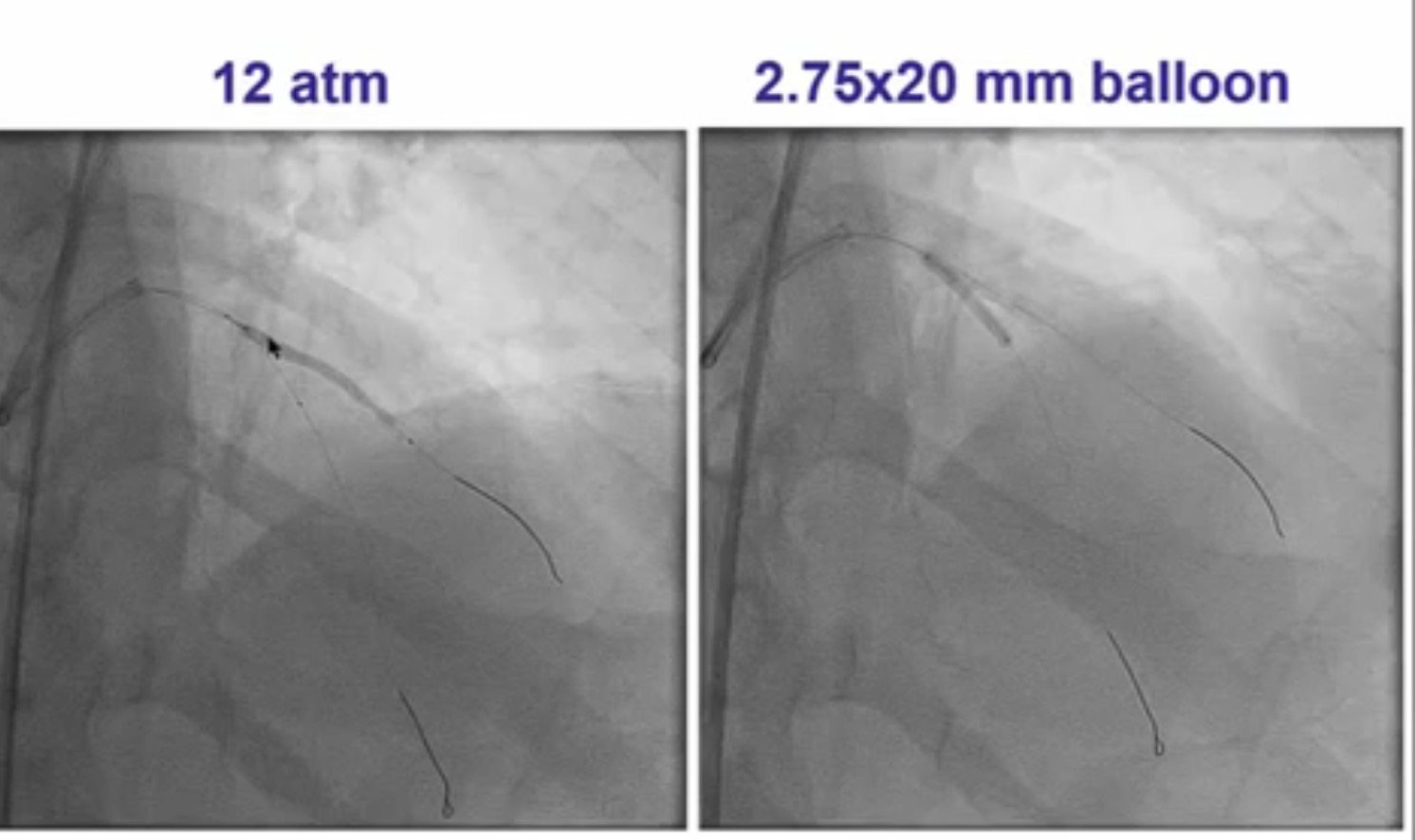
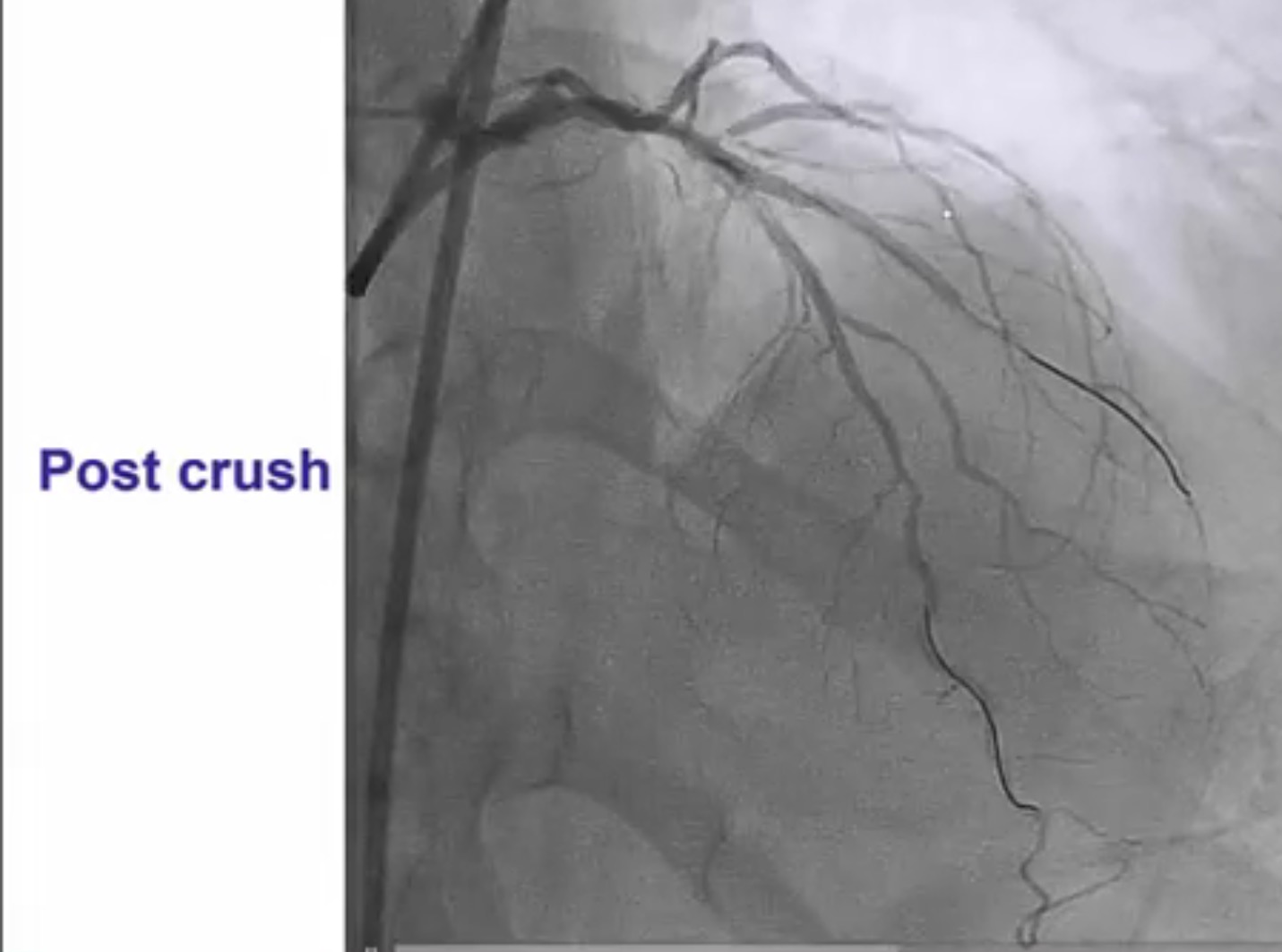
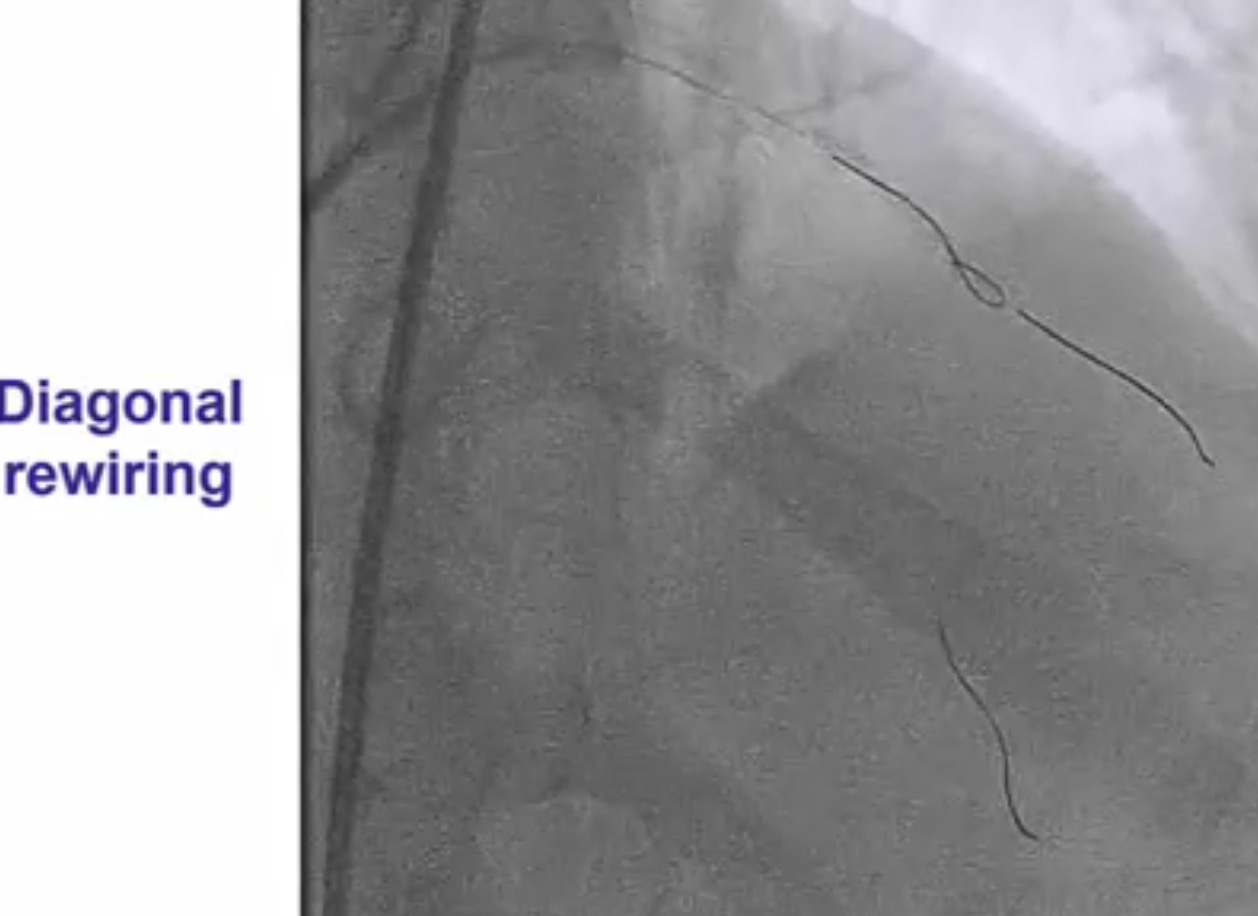
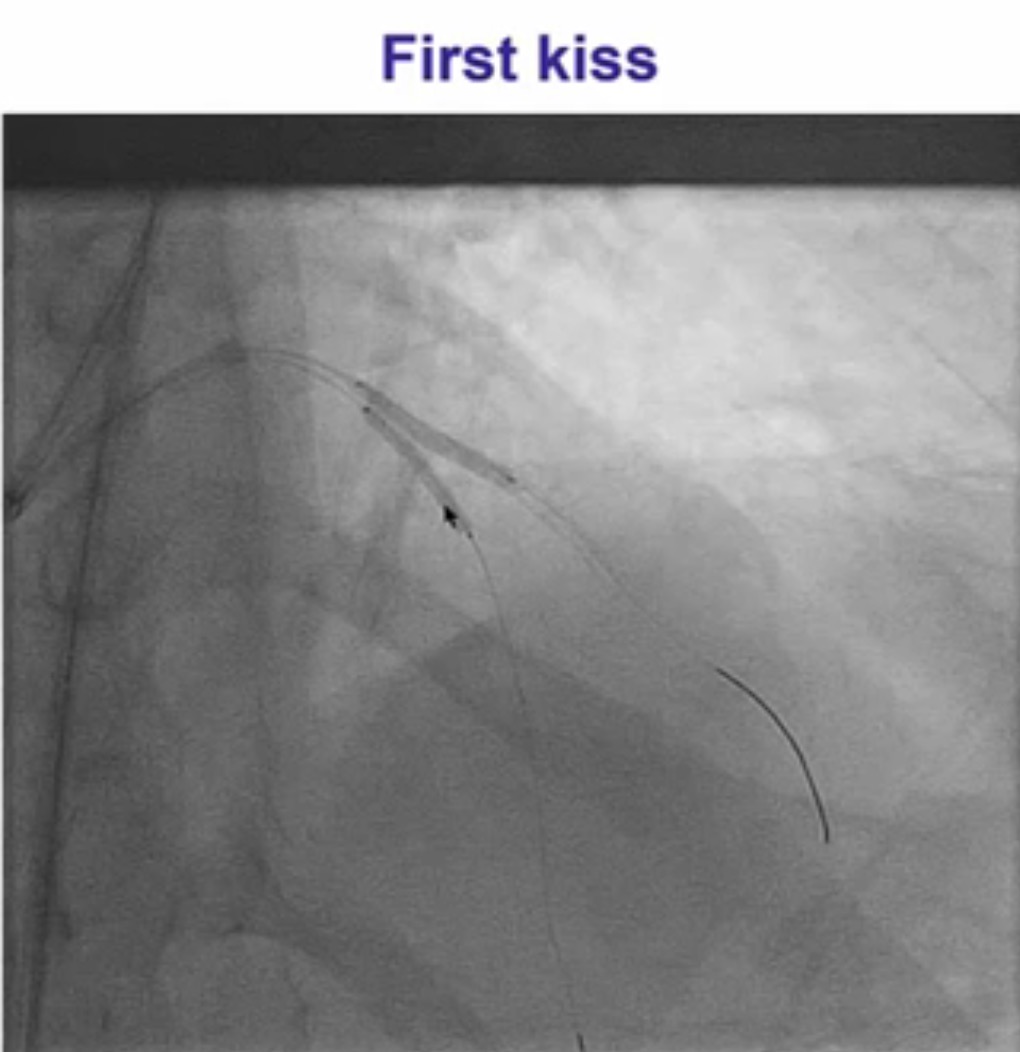
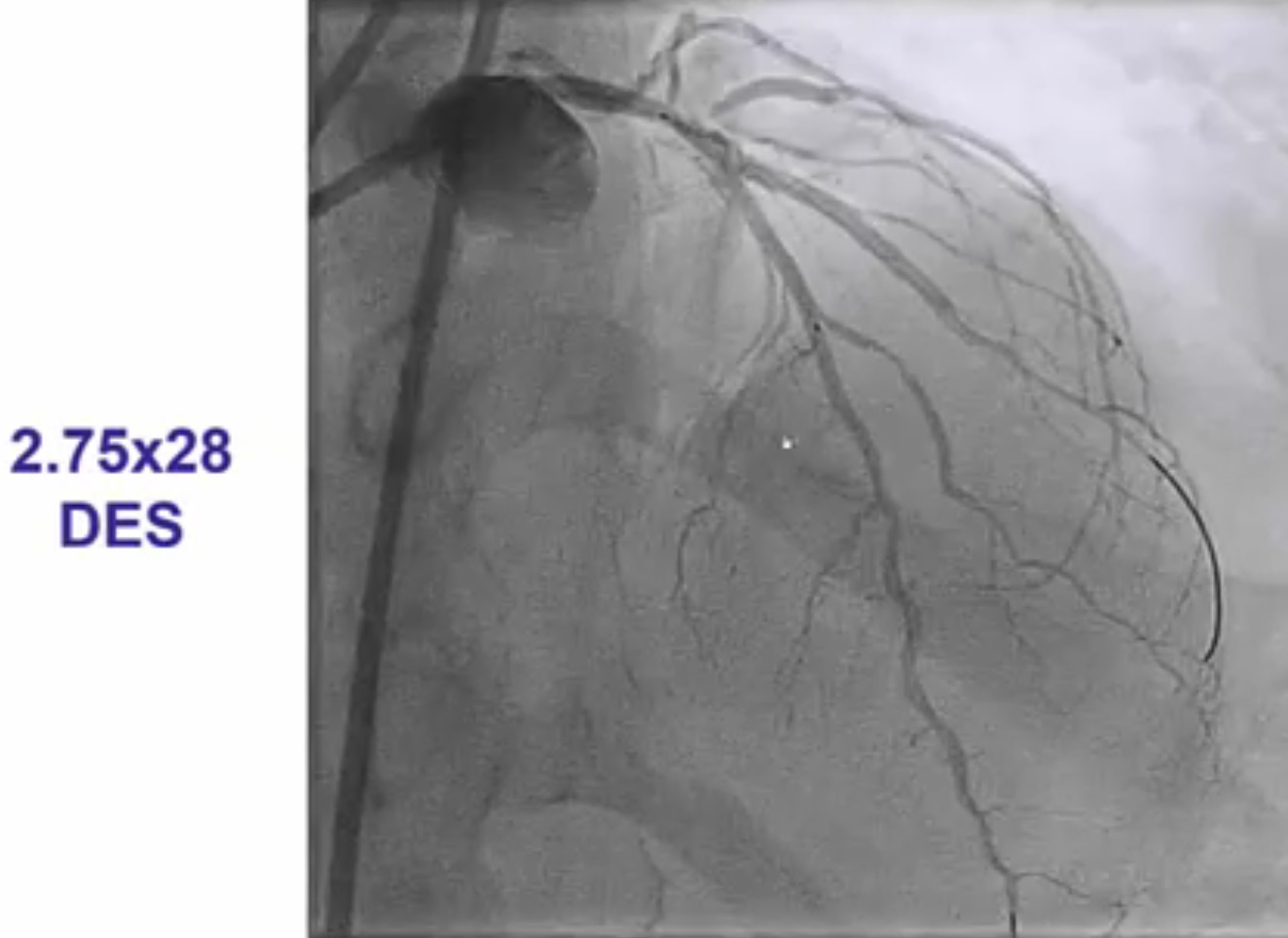
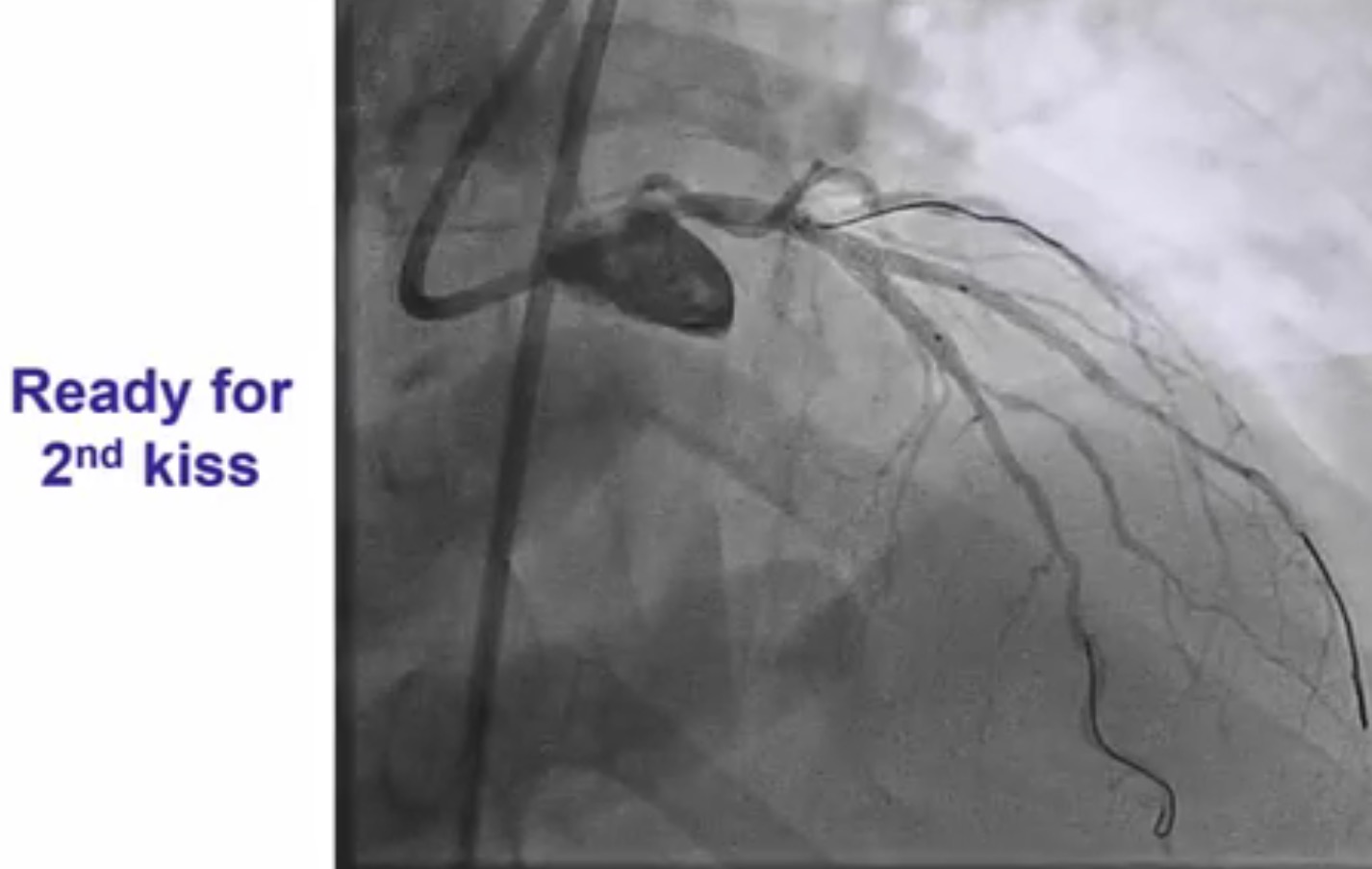
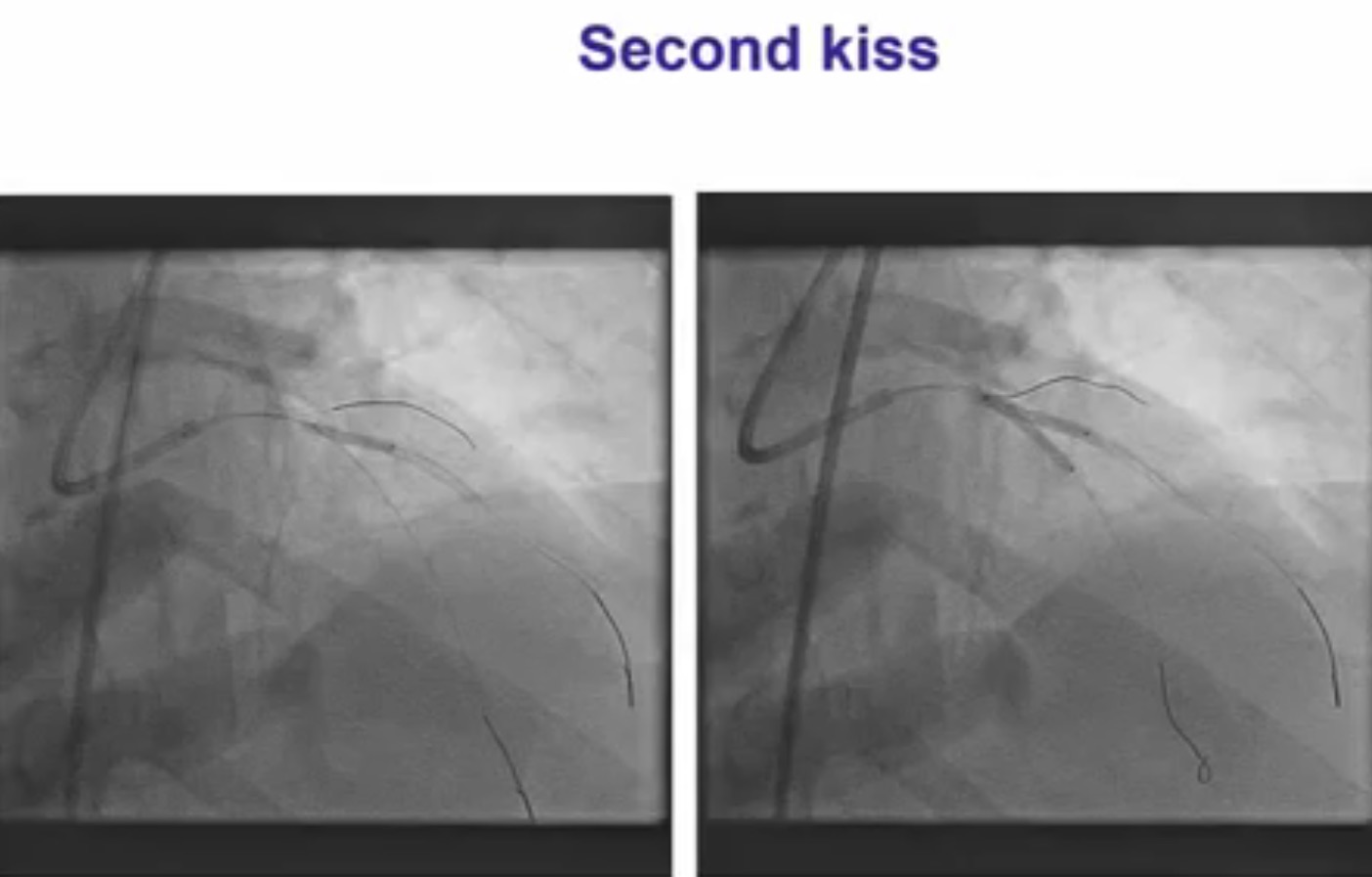
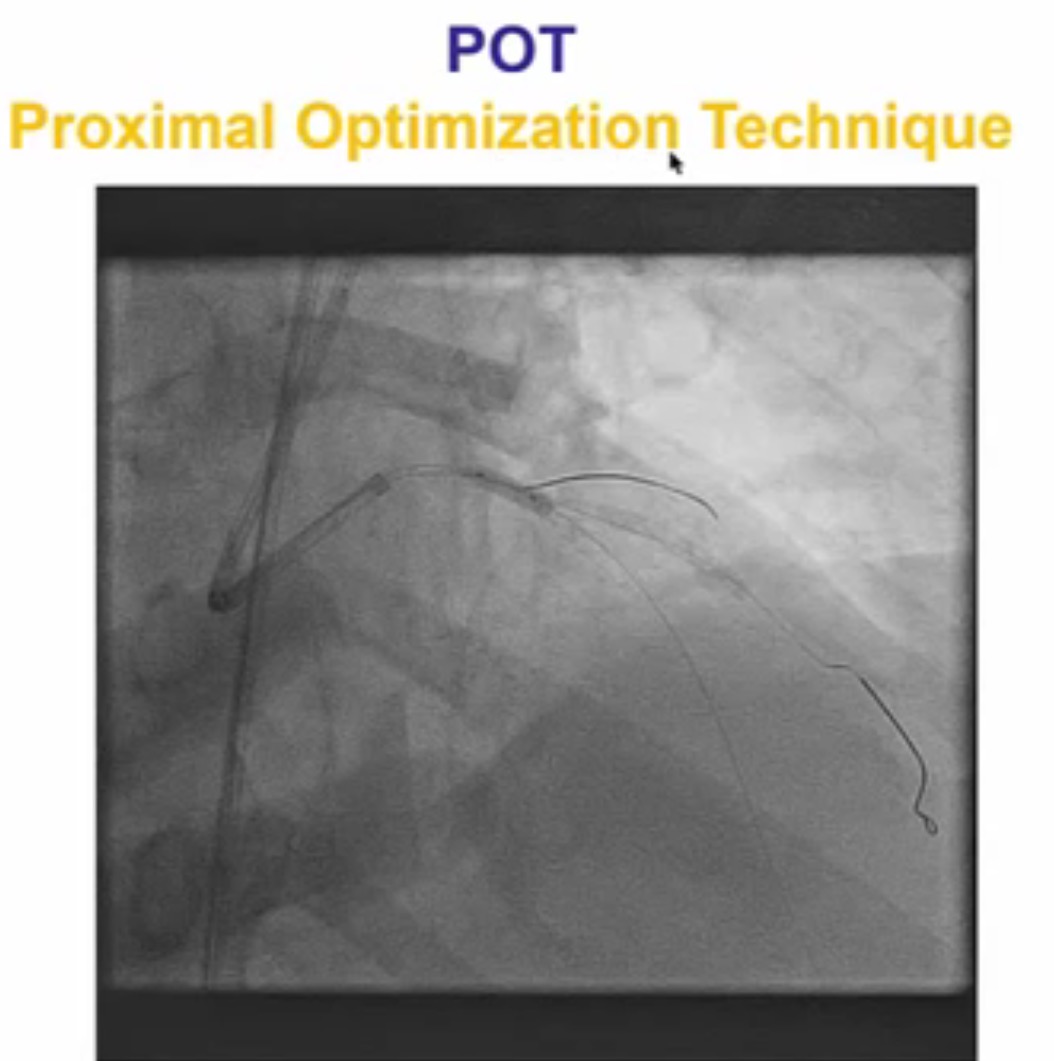
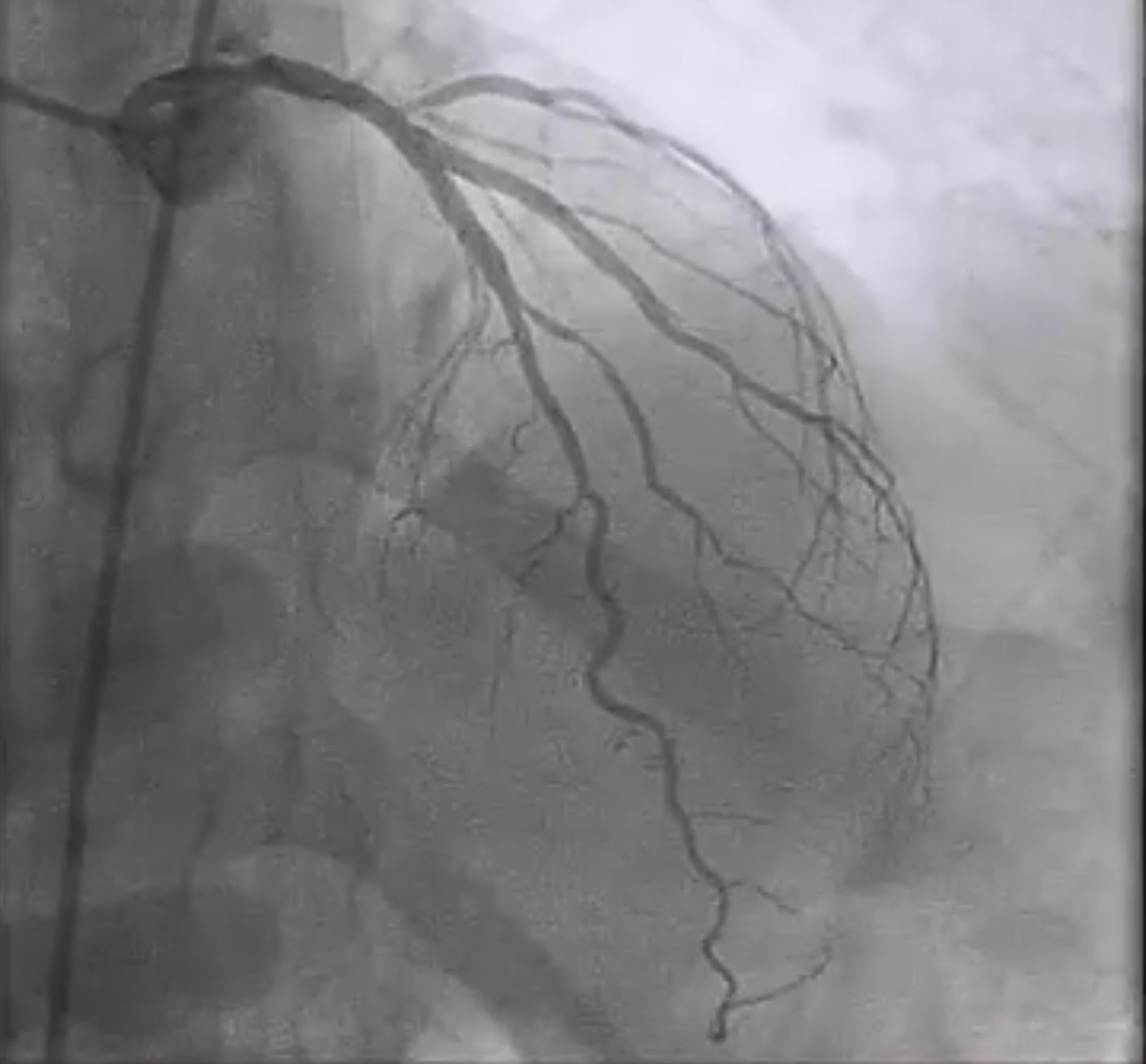
Interventional cardiologists will now need to be familiar with the DK crush technique for left main bifurcation lesions. Both the main branch and side branch have to wired and predilatation is done with a balloon. A balloon of adequate length is placed in the main branch while a requisite drug eluding stent ( DES) is positioned is placed in the side branch with 2-3 mm of its proximal end in the main branch , and deployed at 12 ATM. The side branch stent is crushed by the balloon in the main vessel. A guide wire is negotiated into the side branch and the earlier ( jailed ) guide wire removed from the side branch. The first kissing balloon is done with a balloon in the side branch stent and a balloon in the main branch. The balloon in side branch DES is inflated to 18-20 ATM: kissing is done at 12 ATM. A DES of appropriate size is deployed in the main branch. A new guide wire is negotiated into the side branch through the struts of the main and side branch stents. The second kissing balloon is done with balloons n the main and side branches as before. The side branch balloon is inflated at 18-20 ATM and subsequent kissing done at 12 ATM. The main branch DES is sized by the distal diameter of the vessel. Hence a 2.75 mm diameter DES will be deployed and then the proximal part of the stent is further expanded by a 3 mm ddiameter balloon using the proximal optimisation technique.