{kind=link}
JAMA never stops surprising me. It keeps putting out articles about SARS Cov 2 that are so funny they make me laugh out loud. The papers published on ivermectin have glaring conflicts of interest that are clear as day to everyone but the editors of this medical journal. The ivermectin papers are designed to convince you that, out of the hospital, ivermectin is no better than a lump of sugar in treating COVID patients. Invariably, the drug is given late after symptom onset, on an empty stomach (it should be taken with food) , or the diagnosis of COVID itself is ambiguous. It is well known that the authors have been provided millions of dollars to do the research, apart from either being funded or employed by a company making a competing medicine.
{kind=link}
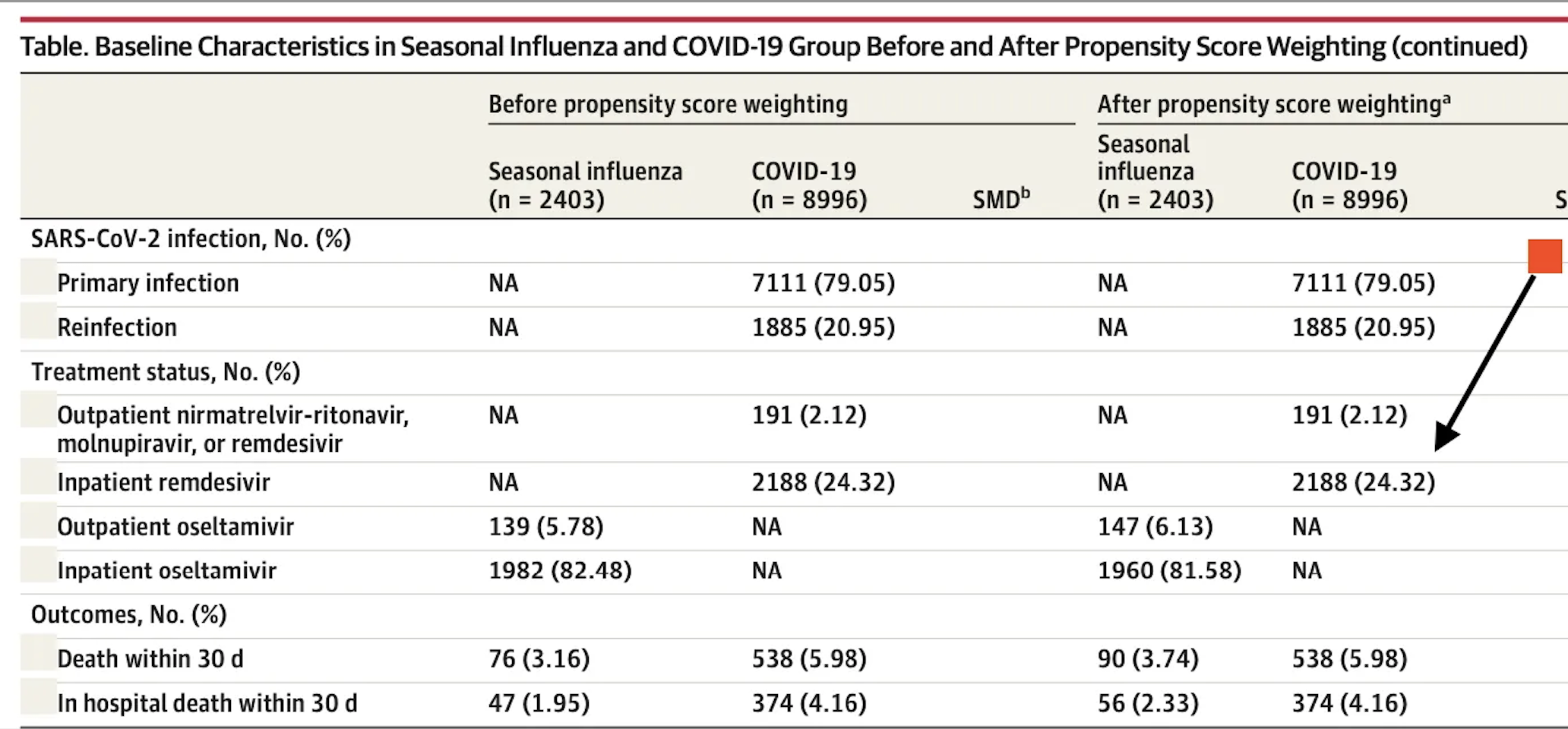
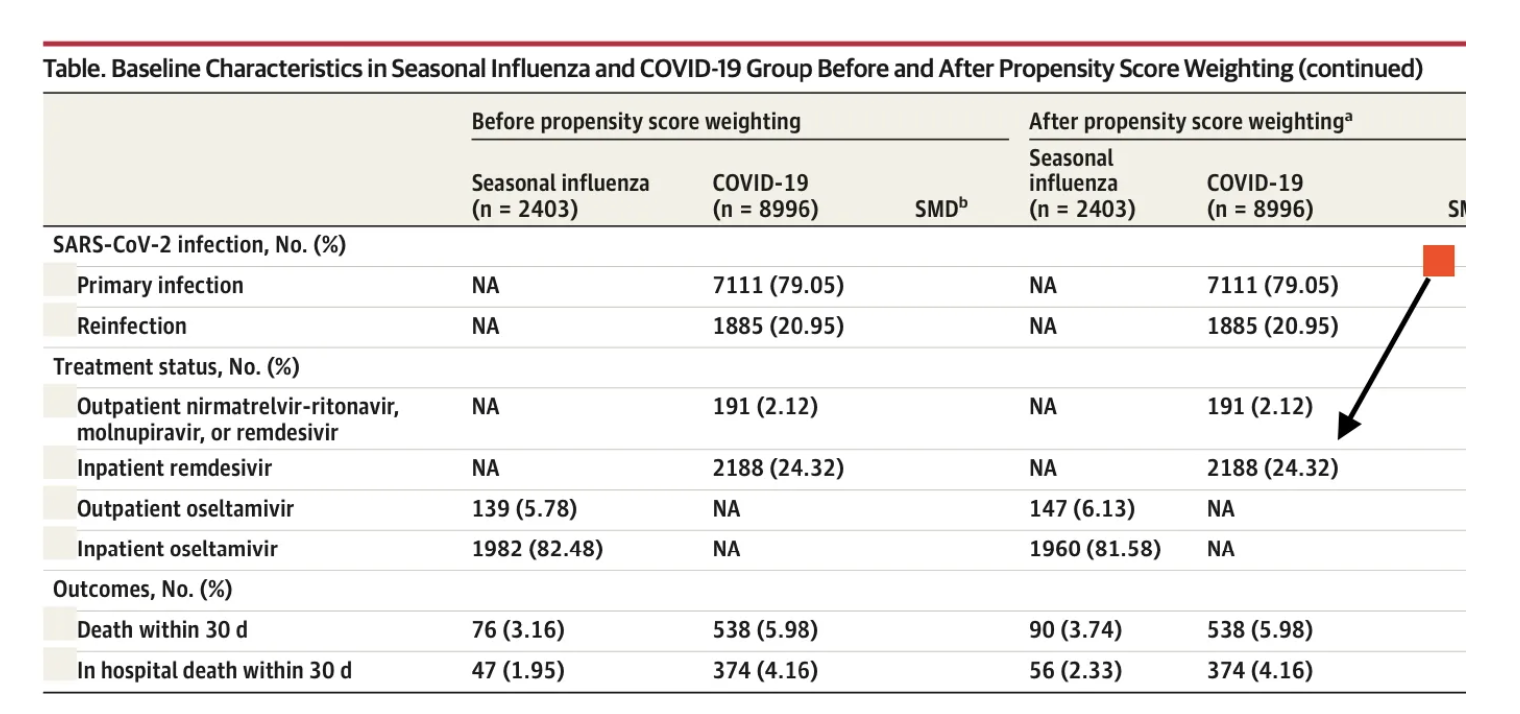
The latest example is a scientific letter that concludes that mortality in hospitalised patients with SARS-CoV-2 is greater than that of those admitted with the flu. This is based on data from the US Department of Veterans Affairs. Elaborate tables are provided with elaborate statistical analysis after propensity score matching of both groups.
But on closer inspection, one realises that more than one fourth of patients received remdesivir. The patients being analysed were admitted at the end of 2022. It is well known that remdesivir killed more than 50% of ebola patients in a study comparing it to other drugs. The paper was published as recently as 2018. Fauci knew that the drug was deadly even as he touted it from within the White House.

A Chinese study found no evidence that remdisivir helped people in the clinic. A French study came to the same conclusion. An NIAID-funded American study too was unable to document a reduction in mortality; all it could accomplish was a quicker recovery by a few days but no significant reduction in mortality. Even the WHO, to everyone’s surprise, reported their SOLIDARITY trial, which also found no clinical benefit with remdesivir. These trials were published way back in 2020 and 2021.
So to find that remdesivir continues to be used in American hospitals is a mystery.
The point that I am trying to make is that when 24% of people in the COVID group are given toxic medicine compared to none in the flu group, there is bound to be a huge confounder. The playing field is already stacked against the poor COVID patients as compared to the flu cohort in terms of mortality.
The conclusion drawn by the authors that COVID is more lethal than the flu is, therefore, null and void. It is not a fair comparison. Crucially, there was no difference in death in those below 65 years. We also have data showing that there has been excess mortality in the USA throughout 2022 and during the months this study is evaluating. Excess mortality is more than 25 percent in some weeks, despite more than two-thirds of the population being vaccinated.
In this study itself, two thirds of people are vaccinated, yet they still land up in hospitals. More than 63% of patients admitted with flu had been vaccinated against it, so it’s not something to write home about. Similarly, almost 55% of those admitted for COVID had received a booster, so clearly the COVID booster is not preventing hospital admission.
Deaths in those hospitalised were greater in the unvaccinated versus those boosted, 8.8% versus 5.2%. But again, concentrating only on this data analysis and not considering world-wide data (showing greater death rates in the vaccinated), the administration of remdesivir to almost 25% of patients and the denial of any repurposed drug have to be factored in.
“The risk of death was higher for people who hadn’t been vaccinated than for those who had been vaccinated or boosted.” These results show how important vaccination is for lowering the risk of death from COVID-19.

The above conclusion by the authors is flawed because of the significant use of remdesivir in COVID patients. Also, being in the USA, none of these patients must have received early treatment for COVID in any form. Nearly 6% of people with the flu got oseltamivir, but only 2% of people with COVID got a monoclonal antibody. Worse, more than 80% of hospitalised flu patients were given oseltamivir, even though most people know that it is pretty much useless after 48 hours of the onset of symptoms. Not one patient with COVID received a single repurposed drug.
The authors do concede that the cause of death in these patients is unclear; this has been the bane of almost all studies done during the pandemic. It has been impossible to confirm whether the PCR tests done in the USA (with inflated ct values hovering at 40) were accurate in diagnosing COVID patients, and there has never been clarity on whether SARS-CoV-2 actually caused the death or was simply a bystander.
Importantly, how does one tease out deaths due to SARS-CoV-2 from the boosters or vaccines administered to these patients? Vaccine-induced injury is reported as high as 3 percent, while autopsy series suggest deaths due to vaccines are as high as 14 percent.
So all things considered, this scientific paper published in JAMA is a feeble commercial for COVID vaccine boosters, but the data provided strongly suggests that vaccines along with boosters are failing to protect against hospitalisation or death. But worse is the fact that American hospitals continue administering one of the most toxic drugs on the market, making the populace sitting ducks by not providing early treatment with cheap repurposed medicines.