Author: admin
POST VACCINE MYOCARDITIS IS REAL AND COULD BE FATAL.
https://www.nejm.org/doi/full/10.1056/NEJMc2109975?query=featured_home
FROM 20 YEARS IN AFGHANISTAN TO 20 YEARS OF VACCINE BOOSTERS AGAINST COVID ?
LARGE INDIAN STUDY SHOWS IVERMECTIN IS VERY EFFECTIVE AS A PROPHYLACTIC AGAINST COVID
I do not manufacture, distribute, or sell ivermectin. I have no stocks in any company that produces ivermectin. I am not in any committee that sets down guidelines regarding covid treatment or management. There are absolutely no conflicts of interest where I am concerned.
But I get disturbed when I read reports of young people in the West who are sent back home to get sicker without being provided any kind of treatment. I get even more disturbed when leading newspapers publish pieces on the sufferings of these young people afflicted with covid. Some of these young people land up in hospitals and even get admitted to intensive care.
What is shocking is that even after more than a year of chaos powerful people are adamant in their stance against ivermectin Actually it will be now 2 years according to credible reports, since the start of the pandemic.
This unyielding rigid stand against ivermectin is not only unreasonable but downright suspicious with so much data of efficacy with ivermectin available in the literature.
I doubt if any doctor in the NIH, CDC, or the White House group has treated a patient with covid.
We now have a large Indian trial including more than 3500 health care workers published in a peer-reviewed journal that reveals a relative 83% reduction in infection with ivermectin prophylaxis. There was in fact a 10% absolute lowering in infection. Cases were confirmed by a PCR test.
Adverse effects were seen in only 1.8%, these were mild, brief, and settled down without hospitalization. Frankly, 2 tablets of ivermectin are just not capable of producing serious side effects. Ivermectin has been used for more than 3 decades.
Symptomatic infection was reduced from 15% to 6%. Is it just lack of empathy or compassion that drives the propaganda against ivermectin, or is something more simple like fiscal benefit?
But will the New York Times, Washington Post, Guardian, Sunday Times, Times of India, or Indian Express bother to do a write-up on this study? Absolutely not. You can be sure they will not touch it.
The New York Times instead, as I say in my video, goes to great lengths to describe how an unvaccinated American young man lands up in intensive care for 11 days. What the newspaper does not explain why this young man was not given any treatment while he languished at home after being found to be covid positive. He was packed off with an oximeter and little or no other advice. He took no treatment, deteriorated at home, and was compelled to arrive to the hospital emergency.
Was any one of the known effective medicines tried on him? No, they were not. Certainly not ivermectin, nor fluvoxamine, nor famotidine. Not even budesonide?
Scaremongering at its very best.
Move over Mr. Francisco Scaramanga. You were fiction buddy, this is for real.
https://www.cureus.com/articles/64807-prophylactic-role-of-ivermectin-in-severe-acute-respiratory-syndrome-coronavirus-2-infection-among-healthcare-workers
RESISTANT HYPERTENSION CAN BE TACKLED WITH A 40 MINUTES BRISK WALK
10.1001/jamacardio.2021.2735
This recent single blind randomised trial shows that there is significant reduction in ambulatory systolic and diastolic blood pressure by walking briskly thrice a week for 3 months in patients with resistant hypertension.
Hypertension is considered “resistant “when blood pressure cannot be controlled with 3 anti hypertensive medicines including a diuretic (water tablet).
Meta-analysis of randomised trials including more than 62ooo patients has already revealed that (in the old) reducing systolic blood pressure by 10 mm Hg and diastolic blood pressure by 4 mm Hg lowers rate of stroke by 30% and acute heart attack by 23%.
Reduction of diastolic blood pressure by 5-6 mm Hg cuts stroke by more than 35% and heart attack by 16%.
This randomised trial published in JAMA reports reduction of office systolic blood pressure of 10 mm Hg after only 3 months of brisk walking , and day time lowering of systolic blood pressure by 8 mm Hg and diastolic blood pressure by 6 mm Hg.
Regular brisk walk or cycling not only reduces high blood pressure but also high blood sugar and increased weight.
So if you suffer from high blood pressure and a doctor advises against a brisk walk or a jog do NOT take him seriously.

TOP GOLFER OUT OF OLYMPICS DESPITE FULL VACCINATION AND DUBIOUS COVID TEST
John Rahm an almost certain medal prospect in the Tokyo 2020 Olympics was disallowed from competing because he turned out covid positive despite full vaccination.
He was found to be positive in June and was forced to withdraw from the Memorial tournament, then.
There are no details of his second covid positive test a month later. Most probably if it was a PCR test, it has picked up dead remnants of the covid virus.
Rahm had to take four PCR tests in the United Kingdom before coming to Tokyo. He failed three consecutive tests as per the Spanish Olympic Committee.
Rahm, as per reports, was administered the Johnson and Johnson vaccine. The explanation provided for the first positive covid test in June was that he competed within 14 days of vaccination.
COVID 19 AND HEART ATTACK FOR THE LAYPERSON

July 29, 2021 https://doi.org/10.1016/ S0140-6736(21)00896-5
The Covid-19 pandemic is being caused by a single strand positive polarity RNA virus named Severe Acute Respiratory Syndrome Corona Virus 2 or SARS CoV-2. The official name was given on 11 February 2020 by the International Committee on Taxonomy of Viruses, and this was announced by the World Health Organisation the same day.
The first cluster of cases was identified in Wuhan, China, but since then almost 200 million cases have become infected by SARS CoV-2, and there have been more than 4 million (forty lakhs) deaths by this virus. India currently carries a burden of 32 million cases with 425000 deaths.
The initial impression had been that SARS CoV-2 only causes pneumonia bit soon it became apparent that there was a multi-system involvement. The virus attacks the lining of small blood vessels called capillaries, this is termed endotheliitis because the lining of blood vessels is named endothelium. Capillary wall inflammation results in multiple small blood clots (thrombi) that compromise blood flow to various organs. The inflammation of capillaries can be caused directly by SARS CoV-2 or by the immune/inflammation reaction it elicits. There are reports that the virus may similarly infect other organs apart from the lungs such as the heart, brain, kidneys, and liver.
There are reports of cardiovascular involvement and thrombotic complications with Covid 19. Infection and inflammation by SARS CoV 2 can increase the risk of heart attack (acute myocardial infarction or AMI) and ischemic stroke. A recent study from Sweden published in The Lancet has highlighted the enhanced risk of acute myocardial infarction and ischemic stroke.
We already know that there is a slight increase in the risk of acute myocardial infarction and stroke with flu, pneumonia, acute bronchitis, and other chest infections. Against this background, Swedish investigators investigated the association if any with Covid 19 and myocardial infarction or stroke. They looked at data from their registers for 86,742 Covid 19 patients with a median age of 48 years and 43% being males.
Two methods for the analysis of data were employed. In the first method, the cases served as their own controls, called the self-controlled case series (SCCS). Here incidence of myocardial infarction and stroke as compared with before and after a patient developed Covid 19 infection. Secondly, they compared the incidence of myocardial infarction and stroke with a comparable group of 348,481 matched controls. The matched controls were similar in age, sex, region along with adjustment for income, education, comorbid disease, and country of birth.
The risk of acute myocardial infarction was about three times higher in the first week after Covid 19, 2.5 times in the second week.
The risk of ischemic stroke was similarly increased by three times in the first week following Covid 19, and by 2.6 times in the second week.
Intriguingly there has been a decline in the cath lab for acute heart attack procedures by almost 30% across the globe. Cities in India too have recorded a reduction in the rate of primary percutaneous coronary intervention procedures (PPCI). The reasons for the observed decline in cases could be an actual reduction in the incidence of acute myocardial infarction brought about by staying indoors during lockdowns or delay in arrival to hospitals by patients with acute myocardial infarction. This delay could be the fear of contracting Covid 19 in hospital, a prospect that cannot be dismissed outright.
The Swedish study reports an increased risk of acute myocardial infarction and stroke soon after Covid 19, but this spike may not be big enough to make up for the lower rate of hospital admissions for heart attack. The Swedish study has estimated excess risk for acute myocardial infarction and stroke at around 0.02%, that is 1-2 cases per thousand.
The independent risk of suffering a heart attack or stroke with Covid 19, however small, cannot be taken casually. The Swedish study is the largest of this kind and hence the data presented is robust. The researchers have noted that the average incubation period is 5 days for Covid 19, and 98% of patients develop symptoms from 2 to 12 days of getting infected.
A study from Denmark has reported an increased risk of acute myocardial infarction following Covid 19 by 5 times, and raised risk of ischaemic stroke by ten times. Covid 19 is associated with a risk of atrial fibrillation that may in turn raise the rate of ischaemic stroke. The risk of stroke has been noted to be 7.6 higher with Covid 19 than with flu.
The higher risks of acute myocardial infarction and ischaemic stroke associated with Covid 19 infection are best explained by direct effects of the virus on endothelial cells and also the heightened inflammatory response that leads to greater coagulability of blood accompanied by exaggerated clumping of platelets. Long-term effects on the cardiovascular system remain to be ascertained.
Apart from the risk of increased ischemic cardiovascular events by Covid 19, there are also reports of direct inflammation of heart muscle termed myocarditis. Contrary to earlier reports, the incidence of myocarditis is low after Covid 19. Myocarditis is best assessed by cardiac MRI that can n to only reveal inflammation of heart muscle but also inflammation of the pericardium, which is the sac enveloping the heart. Again long-term effects of Covid 19 myocarditis are currently unknown because there has not been adequate time for follow-up.
Patients with myocarditis usually present with chest pain accompanied by ECG changes and increased troponin levels in the blood. A 2 D echocardiogram may demonstrate reduced contraction of the left ventricle. But cardiac MRI is best for a definite diagnosis short of endocardial biopsy that may be difficult in many cases, especially if mildly symptomatic. Autopsy series have shown a very low incidence of myocarditis, but these are very sick patients who have died because of Covid 19. Usually, Covid 19 presents with minimal or no symptoms. All heart associations recommend that a sportsperson with confirmed myocarditis should resume training after 3-6 months of symptom onset under the supervision of a physician.
So how does one prevent heart attack during the current pandemic? Firstly one must avoid infection by SARS CoV 2. This is best done by wearing a mask, maintaining distance, and ensuring proper etiquette during coughing or sneezing. Hand washing will also help. Vaccines have been found to be effective in preventing severe disease, hospitalization, and death.
Along with the above, the usual lifestyle adoption is required to prevent cardiovascular disease. Firstly some form of exercise for as little as 20 minutes in a day will go a long way in reducing weight, lowering blood pressure and blood sugar. This could be in the form of a brisk walk, a jog or even a game of badminton. Exercise becomes of paramount importance amid frequent lockdowns that corral up the public.
Blood pressure must be kept in check and optimal blood sugar should be maintained if a person is suffering from diabetes. A healthy low oil largely vegetarian diet cannot be over-emphasized. Crucially, it is imperative that if symptoms of chest discomfort, palpitations, or breathlessness develop a doctor is speedily consulted.
An acute heart attack if not treated quickly can be catastrophic. Nearly 25% of acute heart attack patients die within 30 minutes of onset. There is undoubtedly a credible fear of contracting Covid 19 on visiting a hospital but this must be tempered with the knowledge that an acute heart attack if left untreated could lead to death.
In conclusion, the risk of increased incidence of acute heart attack and ischemic stroke is clear and present in the current pandemic. Covid 19 by itself can directly cause cardiovascular events causing immediate challenges and also for the future. A sedentary lifestyle coupled with the fear of visiting a hospital despite symptoms shall most certainly amplify problems of cardiovascular morbidity and mortality. Tradeoffs are a part and parcel of life and also clinical medicine, we are constantly balancing benefit with risk.
IF VACCINES WORK WHY MASK? IF ASYMPTOMATIC VACCINNEE DOES NOT SPREAD WHY LOCKDOWN ?
https://odysee.com/@drdeepaknatarajan:c/2A60E75F-927E-4001-B448-5273FC9F2288:d?r=5uMQQJcZuB2YfJa7BXcyn1YtoyhPGYTU
1)https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00896-5/fulltext?dgcid=hubspot_email_newsletter_lancetcovid21&utm_campaign=lancetcovid21&utm_medium=email&_hsmi=145089600&_hsenc=p2ANqtz-8OqyYejoHHQkTpsygZYhi1gxeC_T0Emzoq0hL4G95ghWw9jQ59diBpyt0Vj5Pb-NeEPBh3mC_h71k_LmLIQNZRrYGwXQ&utm_content=145016524&utm_source=hs_email
2) https://www.wsj.com/articles/cdc-says-new-mask-mandate-informed-by-cape-cod-outbreak-11627664465
3)https://www.timesofisrael.com/new-high-in-daily-cases-during-current-covid-wave-recorded-friday-expert/
4)https://www.jpost.com/opinion/lessons-cautionary-tale-from-israel-on-the-pandemics-next-stage-675465
ACUTE HEART ATTACK SOON AFTER FIRST DOSE OF mRNA VACCINE
There are now 3 case reports published that describe an acute myocardial infarction soon after the first dose of the Moderna mRNA vaccine.
The first case is a 96 years old lady who had no previous cardiac history. She developed chest pain one hour after being administered the first dose of Moderna Covid vaccine. Her ECG showed ST-segment elevation in the V1 V2 and aVL leads. A bed site ultrasound revealed anterior wall motion abnormality. The patient refused cardiac catheterization and was therefore put on medical treatment consisting of a heparin IV drip. Her troponin was raised. The patient was discharged in a stable condition after 3 days.
The second case, also a woman, developed chest pain within 24 hours of the first Moderna Covid vaccine shot. In the hospital, a bedside ultrasound revealed inferno and lateral wall motion abnormalities. Troponin was raised. Coronary angiography showed a totally blocked left circumflex artery. The patient underwent stenting of the culprit artery.
The second patient was a male who had chest pain with radiation to the, lower jaw soon after the first Moderna vaccine jab. The symptoms began within 24 hours. A CT coronary angiogram revealed a totally blocked left circumflex coronary artery. On invasive coronary angiography in the cath lab there was a 90% block in the left circumflex artery that was predicated and stented.
Excellent antegrade flow was achieved in both cases.
The take-home message is that albeit an acute heart attack is uncommon post-vaccination it must always be kept in mind if a person develops chest pain soon after the first dose of the Moderna mRNA vaccine against Covid 19. The exact pathogenesis remains to be established, but these 3 cases presented with a thrombus in their culprit vessel.
But the question remains, what exactly triggered the thrombus in the culprit coronary artery?
IF ONLY SOMEONE HAD TOLD PIERS MORGAN ABOUT IVERMECTIN
https://odysee.com/@drdeepaknatarajan:c/PIERS:3?r=5uMQQJcZuB2YfJa7BXcyn1YtoyhPGYTU
It is more or less clear that the effectiveness of vaccines is dwindling substantially after 6 months, and this must have been known to the companies that manufacture them. The level of antibodies against the Astra Zeneca (AZ) vaccine is markedly lowered after a mere 70 days, as published in the Lancet.
Public Health England has published data (in the NEJM )that the effectiveness of the AZ vaccine against the Delta variant is less than 70% and around 88% with the Pfizer vaccine.
University College London suggests that effectiveness is just 0% against mild infection and 60% against severe infection.
The Israeli health ministry has acknowledged a study that effectiveness against serious infection against the delta variant is around 50% in those over 60 years. This is understandable as old people are unable to ramp up antibody production.
None of these studies have measured T cells or memory B cells that may endure much longer and tackle the severe infection. On the field, however, breakthrough infections are on the rise.
Against this information we now learn from there noted British journalist Piers Morgan that he contracted the Covid 19 virus in the Euro Cup finals between England and Italy. He developed a high fever accompanied by cough and body aches. One of his favorite wines tasted like “rusty water” because of his loss of smell and taste. Albeit he is on the road to recovery his doctor has advised high dose corticosteroids to prevent “long covid.”
There is no randomized trial on high-dose corticosteroids to prevent long covid. Or is that despite 2 jabs of the AZ vaccine Piers still managed to get severe Covid.
Piers also mentions Andrew Marr (with the BBC) who contracted the virus in the G7 Summit despite, yes, 2 vaccine jabs. I do not have the details of the gravity of Mr. Marr’s illness.
The fact remains that 2 vaccine jabs are no guarantee against contracting C -19. Which brings us to the question as to why Piers was not offered effective early treatment for his illness. It is time that Piers does some research on ivermectin, fluvoxamine, and anti-androgen drugs.
It would do the community and people at large on the planet if Piers writes on ivermectin or the impact of early treatment. Common sense dictates that if the virus is tackled within 2-4 days there is very little possibility of any immune reaction developing in the future.
I have a soft corner for Piers because I have watched him face 6 balls (ouch !) from Bret Lee, one of the fastest bowlers emerging from Aussie. Bret could easily touch 150 K/hour in his peak, and that is faaaaast. If nothing else Piers has guts. The over may not be in the league of a Shoaib Akhtar bowling to Sachin Tendulkar, Malcolm Marshall attacking Sunil Gavaskar, or Dennis Lillee hurling a cork ball at Vivian Richards, but it is still worth watching. “Bring it on” urges Piers after being struck by Bret Lee, some pluck.
If only Piers had been provided ivermectin right away on the 13th or 14th of July. Here is wishing him complete recovery from the damn virus.
AVOIDABLE DEATH OF NEIL ARMSTRONG, THE FIRST MAN ON MOON
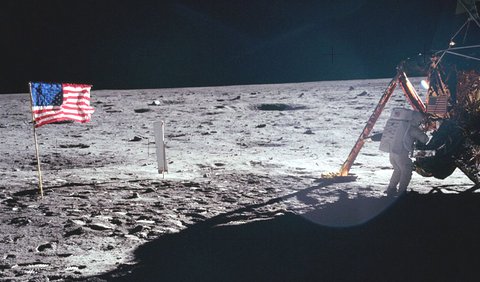
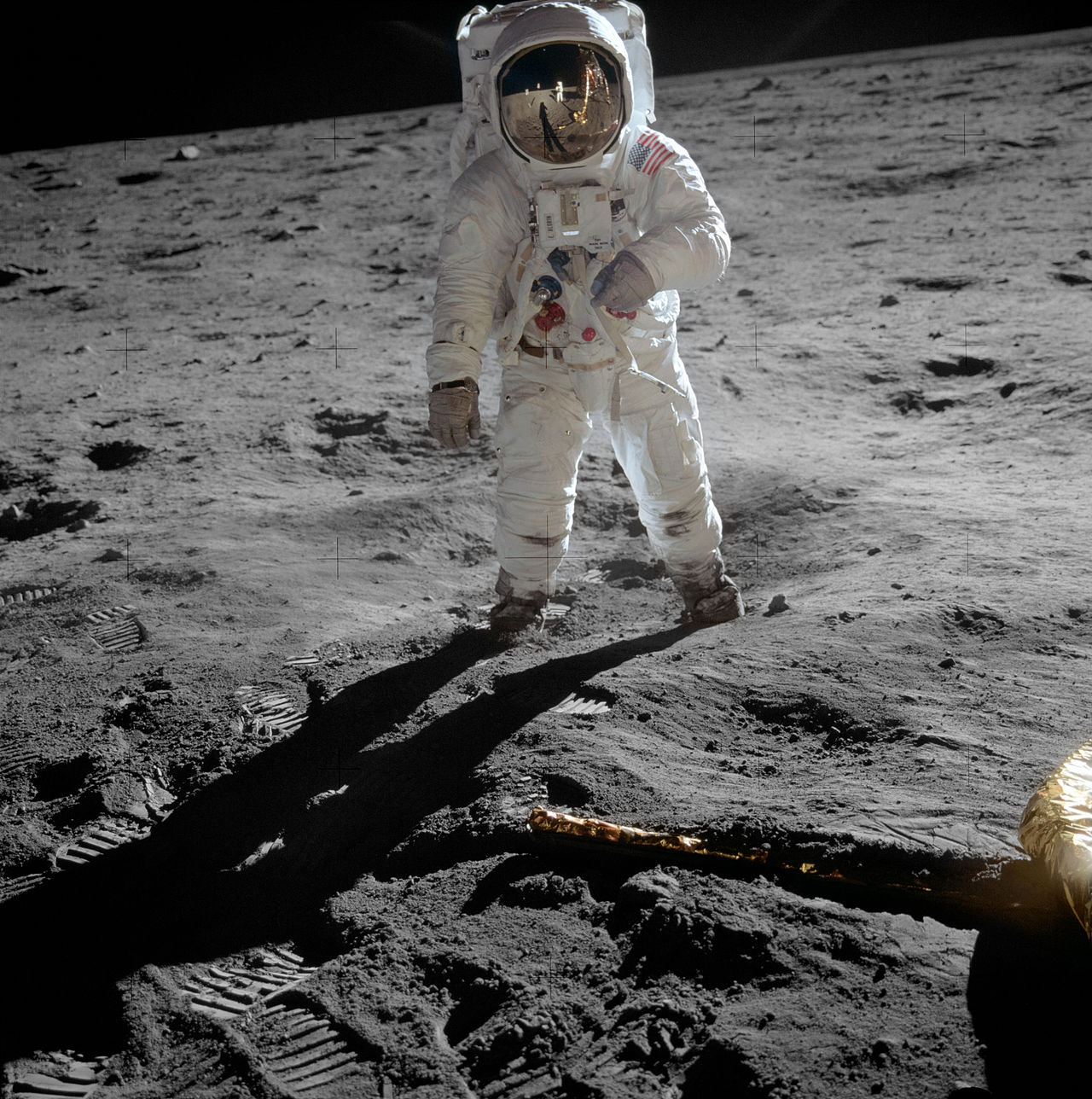
The first man to set foot on the moon was Neil Armstrong, way back on 20th July 1969. Neil Armstrong was an ace pilot and an engineer who supervised the Apollo 11 mission, which was the first space project to land on the moon. He became following this probably the most famous man on the planet. I still remember the grainy pictures beamed on our TV at home of him and Buzz Aldrin hopping on the moon’s surface. The famous line was uttered that “That’s one small step for man, one giant leap for mankind.” This was from more than 240,000 miles away. Possibly Armstrong dropped “a” before “man” or maybe he did not.
Just as famous was the line radioed back to mission control “The Eagle has landed,” when the lunar craft finally descended on the surface of the moon.
The Apollo 11 mission took off using a huge Saturn V rocket standing 363 feet. There is a documentary “Apollo 11” and also a terrific film “First Man” that has Ryan Gosling portraying Armstrong. Armstrong despite his immense fame did not care too much for grandiose pronouncements or striking statements powered by grand eloquence. Armstrong throughout his life remained a perfect gentleman with his feet firmly on the ground. This was an extraordinarily humble man right till the end. But what an end!
Few in India know that Armstrong died because of an easily avoidable error made by a nurse. Armstrong underwent a CABG surgery in early August of 20112. The surgery was unremarkable and Armstrong was recovering pretty well, he had even begun to walk following the operation. A nurse removed the temporary pacing wires attached to Armstrong’s heart in the ward itself. Sadly this tore apart heart muscle and there was instant severe bleeding into the pericardium (sac lining the heart) and hypotension. He was shifted to the catheterization laboratory where attempts were made to revive him, but had to be transferred to the operation room where all attempts at salvaging him failed. Armstrong lingered for another week before he died.
Temporary pacing wires are often attached to the surface either the right or left ventricle, and also the atrium. They are secured by a curve at the tip with or without a stitch. This is done during surgery. The wires are usually pulled on the 3rd to 5th postoperative days. Actually many surgeons prefer not to pul out the wires but just cut them on the surface of the skin. There is always the small risk that when the wires are tugged the heart wall can be ripped open, whether it is the ventricle or especially the atrium. Armstrong must have been on blood thinners ( aspirin).
Temporary epicardial pacing wires are placed to tackle postoperative arrhythmias that have the potential for hemodynamic instability. Pacing wires have been used to suppress atrial and ventricular tachyarrhythmias, as also as a safeguard in case heart rate drops after surgery. There may be rare complications, which can be deadly, as what happened with the first man to step on the moon. The most common complication is that the wires do not work when needed. Importantly removal of these wires can result in injury to venous grafts and tear of the chamber to which the wires are attached. The result is bleeding into the pericardium accompanied by a severe and sustained drop in blood pressure (also called cardiac tamponade).
Certain patients, however, may not require these temporary pacemaker wires, patients who undergo off-pump CABG, and those who already have a permanent pacemaker. There have been studies done trying to discriminate patients who could be at high risk for a temporary pacemaker. Diabetes and pre-operative arrhythmias are strong risk factors, and if the pacing was needed as the patient came off bypass. Most centers using bypass during CABG continue to place temporary pacemaker wires. Temporary epicardial pacing wires are also placed routinely during valve surgery, but high-risk patients can be teased out before surgery. Postoperative support if required is for 1 to 2 weeks.

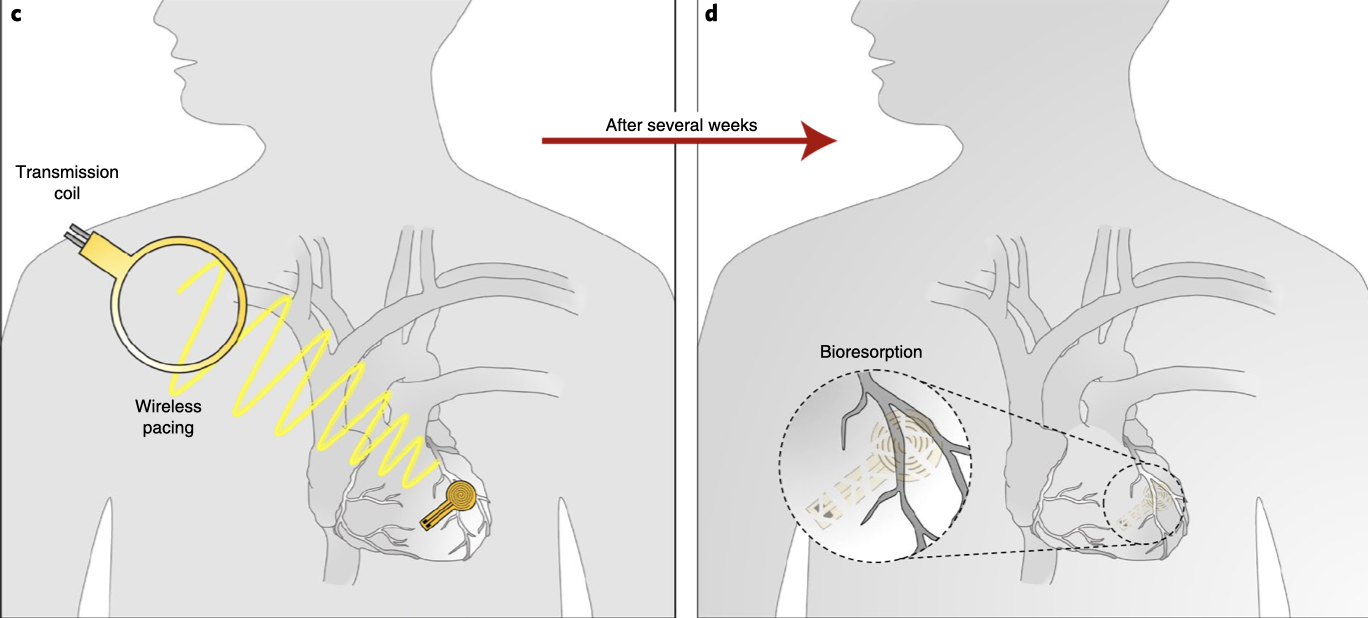
The good news is that now we are on the cusp of using a pacemaker that can dissolve within a month or two after the operation. A fully implantable, bioabsorbable pacemaker that can pace the human heart is being developed. Animal studies have been successful. There will be no possibility of infection or any complication during yanking of pacing wires. This device is very small and made of water-soluble biocompatible materials. It has no wires or battery. It will do its work of protecting the patient from possible arrhythmias and melt away. The device is 16 mm in width, 15 mm in length, and weighs just 0.3 g. The device is capable of receiving commands and power from an external source on top or a few inches from the heart. It has successfully captured and paced rabbit and mouse hearts. The pacemaker largely dissolves by 3 weeks and almost completely by 12 weeks.
The dissolving pacemaker is stitched on the surface of the heart and therefore there is no risk of a residual fragment traveling in the bloodstream. Human trials are eagerly awaited. The future looks promising but one must bear in mind the usual caveats of suboptimal effectiveness and unanticipated adverse effects. Till then we will have to continue with the temporary epicardial pacing wires attached to an external generator.
The richest man in the world , Jeff Bezos, went up 65 miles above Texas ,yesterday. It was a gigantic unadulterated ego trip lasting 11 minutes, even as millions on the ground stared into a dark abyss infested with the Covid 19 virus.
PARADISE LOST WITH SACUBITRIL/VALSARTAN

The combination of an angiotensin receptor blocker and a neprilysin inhibitor (ARNI) made a spectacular appearance with the large randomized Paradigm trial showing the significant lowering of mortality and hospitalization when compared with valsartan alone, in patients with heart failure with reduced ejection fraction (HFrEF). The ARNI used was a molecule that contained sacubitril and valsartan. There was an absolute 4.7% absolute reduction in events. Many physicians embraced ARNI in treating patients with HFrEF based on these results. The drug has been introduced in India and is replacing angiotensin-converting enzyme inhibitors in the management of heart failure patients. PARADIGM was a large study that included more than 8000 patients with HFrEF.
ARNI was next employed in another large randomized trial with about 5000 patients with HFpEF or heart failure with preserved ejection fraction. This was named the PARAGON trial. These patients (NUMBER 4822) had a left ventricular ejection fraction of 45% or more, raised levels of natriuretic peptide, and structural heart disease. In PARAGON there was no difference in hospitalization and death from cardiovascular causes with ARNI in patients with HFpEF.
A case was however made by the manufacturing company that certain subsets benefited with ARNI, namely female patients and those with a lower ejection fraction. This seemed more of a spin because HFpEF is a heterogeneous disease with multiple causes that defy shoe fit all approach. Also currently it is estimated that a significant proportion of patients with HFpEF suffer from cardiac amyloidosis that cannot possibly improve by an ARNI.
Recently another double-blind active-controlled randomized trial comparing ARNI with an old angiotensin-converting enzyme inhibitor in patients with HFrEF soon after acute myocardial infarction has been presented in the recently concluded ACC meeting. Patients included had to have an ejection fraction of 40% or less and /or pulmonary congestion. More than 5600 patients were randomized within a week of acute myocardial infarction to either an ARNI or ramipril. This is the PARADISE-MI trial that included patients on an average 4 days after myocardial infarction. The average ejection fraction was 37%. Sacubitril/valsartan 200 mg was matched with 5 mg ramipril, both drugs being given twice a day, along with standard post-heart attack treatment.
The mean age is 64 years and a quarter are women in this trial. Almost 90% underwent PCI. More than 90% of patients received dual antiplatelet and statin therapy. Beta-blockers were administered to 85% while an aldosterone antagonist was given to 40% of patients.
There was no difference in clinical outcomes in patients receiving ARNI or ramipril. The primary outcome of cardiovascular death, first heart failure hospital admission, or outpatient heart failure remained the same in both groups. Sacubitril/valsartan failed in significantly lowering the rate of CV death, heart failure hospitalization, or outpatient heart failure needing treatment.
The researchers rightfully assert that albeit ARNI did not show superior results in patients with reduced ejection fraction soon after myocardial infarction, it was as safe as ramipril. Possibly an ARNI is more effective in sicker patients with chronic heart failure than when used as a preventive strategy soon after myocardial infarction.
The big problem is the prohibitive cost of sacubitril/valsartan as opposed to that of ramipril. The cost of 10 tablets of 2.5 mg ramipril in India is Rupees 30 only, whereas 14 tablets of ( 24mg/26 mg) ARNI (Wymada) will cost at least around Rupees 880.
Now considering that there is little or no difference in clinical outcomes between ARNI and ramipril in patients with heart failure soon after acute myocardial infarction, ramipril may turn out to be the winner, even though around 10% of patients could develop persistent cough leading to discontinuation.
The PARADISE trial is a good example of corporate pressure on the medicine market in patients with heart failure. The spin is quite obvious. The aim is to use an ARNI in as many patients as possible, much like the mass vaccination drive in children. Children get a much less severe infection, rarely die, and transmit the Covid 19 virus far less than adults. This is the reason why the UK government has opted not to mass vaccinate children and to do so only in the vulnerable ones keeping in mind the development of myocarditis soon after the second mRNA jab in children, particularly boys. The risk-benefit ratio in vaccinating children remains blurred, and therefore ideally one must wait for more data before launching a mass vaccination drive in the young ones.
Vaccinating vulnerable adults is more in line despite significantly reduced efficacy against the Delta variant in Israel, and mounting new cases in high vaccinating countries such as the UK and Holland.
Coming back to the topic concerned sacubitril/valsartan failed to trump good old ramipril in patients with acute myocardial infarction and reduced left ventricular ejection fraction. Ramipril can hence be a suitable alternative in post myocardial infarction patients with reduced left ventricle function or pulmonary congestion.
IVERMECTIN CAN BAT ALONG WITH VACCINES; THE GUARDIAN SHOULD NOTE
The Israeli prime minister notes that the Pfizer vaccine is significantly less effective against the Delta variant.
The English health secretary reveals he is infected by C19 despite full vaccination; implying that because he has “mild” symptoms the vaccine has mitigated the intensity of the infection or that the vaccine really did not help much.
Countries with the highest per capita vaccination are experiencing a surge by the Delta variant.
In India, however, 4 states ( Uttar Pradesh, Uttarakhand, Goa, and Karnataka have decided to promote ivermectin as a prophylactic for good reasons.
Most Indian physicians in India who have treated C19 patients with ivermectin are impressed by its effectiveness.
Every patient with Covid that I have treated with Ivermectin recovered within a few days. The oldest gentlemen were 78 and 80 years, both had diabetes.
Vaccination should be restricted to the vulnerable and till fully vaccinated should use ivermectin for prevention.
The Guardian would do itself credit by seeking the opinion of Indian physicians who have actually used ivermectin to treat patients with Covid 19.
VERY LOW PREVALENCE OF HEART INFLAMMATION IN ELITE ATHLETES WITH COVID.
Data on 789 professional athletes infected with Covid 19 reveals that only 0.6 % suffered inflammation in the heart, that is 5 of 789.
Also none of these athletes had moderate or severe Covid 19, underlining the fact that the young do not get severe C 19 infection.
The average age of the cohort was 25 years and 98% were males. They were tested around 19 days after symptom onset.
27 athletes underwent cardiac MRI that showed inflammation in only 5 of the 789 (0.6%).
Resumption of training and competition should be delayed by 3- 6months in the presence of heart inflammation.
https://jamanetwork.com/journals/jamacardiology/fullarticle/2777308?guestAccessKey=62e0897e-544a-4abe-b41e-401983df9ec4&utm_source=silverchair&utm_medium=email&utm_campaign=article_alert-jamacardiology&utm_content=etoc&utm_term=071221
RECENT META-ANALYSES OF RANDOMISED TRIALS WITH IVERMECTIN NEED MORE EXPOSURE BY THE MEDIA
Two recently published meta-analyses of randomised trial with ivermectin in patients with Covid 19 have shown significant reduction in mortality. Lower levels of inflammatory markers ( d Dimer, CRP and ferritin) have been associated with ivermectin , as also quicker clearance of C19 virus.
Strangely there has hardly been any stir in the Western press; it is difficult to fathom the reasons. Hopefully the Indian press gets more excited.
The 2 trials need exposure, especially considering “breakthrough” infections despite being fully vaccinated against the Delta variant.
It is obvious that more C 19 variants shall keep popping up.
1)Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines
American Journal of Therapeutics 28, e434–e460 (2021)
2) Meta-analysis of randomized trials of ivermectin to treat SARS-CoV-2 infection
Published by Oxford University Press on behalf of Infectious Diseases Society of America.

POST mRNA JAB MYOCARDITIS IS CHILD’S PLAY; WHAT COULD POSSIBLY GO WRONG ?

https://odysee.com/@drdeepaknatarajan:c/POST-mRNA-MYOCARDITIS:c?
(ON ODYSEE.COM)
Numerous series of myocarditis following the second jab of an mRNA vaccine have been published in leading peer-reviewed journals. The common theme is that young men develop myocarditis within 3-5 days after the second jab, most have severe chest pain, elevated troponins suggesting heart muscle cellular damage, ECG changes, signs of heart inflammation on cardiac MRI, and reduced left ventricular ejection fraction on 2 D echocardiogram. One patient had an ejection fraction as low as 35%. All these patients needed hospitalisation. The researchers report that number of cases was much greater than normally observed.
The verdict however is that myocarditis is “rare”, “mild” and the benefits of vaccination outweigh the risks in children.
Against this background, we have a news report in the Times of Israel that more than 75 schoolchildren have contracted (delta) Covid 19; it began with one schoolchild getting infected by a vaccinated relative, who in turn got infected by a vaccinated person returning from the UK.
The Israeli government may reimpose restrictions starting next week. The moot point is whether vaccines are ineffective against Delta or whether the Israeli government wants to motivate more people to get vaccinated, especially children.
CRISPR-CAS 9 SYSTEM SUCCESSFUL IN FIRST EVER TRIAL IN INHERITED TRANSTHYRETIN AMYLOIDOSIS
https://odysee.com/@drdeepaknatarajan:c/A:6
Amyloid is an abnormal protein that infiltrates the heart, kidney, liver, and nervous system.
When deposited in the heart it causes right heart failure, heart block, and ventricular tachycardia.
Cardiac amyloidosis is a fatal disease that substantially shortens one’s life span to 2 to 6 years.
Cardiac amyloidosis, however, is not a rare disease.
15% of “low flow low gradient aortic stenosis “patients have cardiac amyloidosis.
15% to 30% of patients with diastolic heart failure have cardiac amyloidosis.
Cardiac amyloidosis is diagnosed by ECG showing small QRS complexes, by 2D echo showing thickened ventricular walls, thick interatrial septum, and thickened valves. There is also evidence of reduced ventricular filling.
Cardiac MRI shows patchy late gadolinium enhancement.
There are 2 kinds of amyloidosis, one caused by light chain immunoglobulins, and the other is TTR or transthyretin amyloidosis. TTR amyloidosis can be either acquired or inherited.
Inherited TTR amyloidosis is due to more than 100 mutations in a TTR gene in the liver.
Drug therapy for TTR amyloid has not been too successful.
The NEJM last week published a pilot study in 6 patients with inherited TTR amyloidosis. This is a landmark trial because this is the first time the CRISPR-Cas9 system has been used in patients with inherited TTR amyloidosis.
An IV injection with a CRISPR- Cas 9 gene editing system was given. This is a complex of a guide RNA and Cas 9 enzyme in a nanoparticle. The guide RNA carries the gene-editing enzyme Cas9 to the gene in the liver, where it cuts the TTR gene. The cut gene can no longer produce TTR protein.
In 28 days there was an 87% reduction in TTR levels, one patient had a decline of 96%.
Adverse effects were mild, few, and brief. Only a single shot is required.
It is imperative of course that more trials are done to confirm the safety and efficacy of this pilot study using the CRISPR-Cas 9 system, which was discovered in a bacterial immune system.
The Nobel Prize in Chemistry (2020) was awarded to two women scientists who transformed a bacterial immune mechanism, commonly called CRISPR, into editing the genomes of everything from wheat to mosquitoes to humans.
The award went jointly to Emmanuelle Charpentier of the Max Planck Unit for the Science of Pathogens and Jennifer Doudna of the University of California, Berkeley, “for the development of a method for genome editing.”
https://www.nejm.org/doi/10.1056/NEJMoa2107454
THE IVERMECTIN OXFORD TRIAL NEEDS REDESIGNING TO GET CREDIBLE RESULT
I have been working in hospital and the cath lab right through the Pandemic. After considerable deliberation I took 2 shots of the ChAdOx1 vaccine. I have a number (provided by the Indian government) to prove this, and therefore I am not an anti-vaxxer. I am not in the habit nor in the business of misinformation. I am an interventional cardiologist in the vulnerable age bracket and considered vaccination well worth the risk.
But with children the risk benefit ratio does not work very well, and I would wait for more evidence before embarking on mass vaccination in the little guys.
They have had a torrid time the last one and a half years. No school, no education, no sport, no friends, in fact no nothing. Worse they do not have a spokesperson defending them or their cause.
Oxford investigators in the PRINCIPLE platform are about to begin a randomised trial with ivermectin. Their protocol for the trial, however, leaves must to be desired. It seems so skewed against ivermectin that it is bound to fail.
In India, and Delhi in particular, Iveremectin is used at a dose of 400 to 500 micrograms per Kg for at least 5 days if not longer. Crucially it is supposed to be administered at the earliest, within 3-5 days from symptoms onset for best results.
The PRINCIPLE investigators on the other hand will wait for 14 days from onset of symptoms and use a small dose of 300 micrograms per Kg for only 3 days. This obviously will be suboptimal. Importantly patients who are quite sick will be recruited, those above 65 years, or if younger with some chronic condition such as heart, lung, liver, or neurological disease.
It is imperative that the Oxford investigators redesign their methods for the Ivermectin trial to obtain truer results. The dice,in their trial, appears to be loaded against ivermectin.
VACCINE INDUCED IMMUNE SELECTIVE PRESSURE COULD ENHANCE COVID VIRUS MUTATION
YouTube odiously continues to pull down videos on ivermectin, even as the evidence for efficacy mounts by the day. The latest meta- analysis based on a meta analysis of more than 21 randomised that included more than 2,700 patients , reports that there is low and moderate certainty that ivermectin cuts death rate by significant 68%. Also there is low certainty evidence that ivermectin reduced infection by a significant 86%, that means if ivermectin taken once a week could prevent infection as much as the best vaccine.
Ivermectin has to be kept in mind against the background of rapid development of variants of concern. A theory currently being proposed is the concept of immune selective pressure. This is the pressure mounted by a vaccine on the virus that compels the virus to transform or mutate. In between 2 shots of a spike focussed vaccine, there is production of antibodies but antibodies produced are not effective enough to fully neutralise the invading virus. The antibodies are not fully developed. The virus now has the time, space, and luxury to mutate and evolve into new variant, which can infect a cell with greater ability and also evade immunity. Worse, a variant of concern can be more virulent and deadly. The recent fiasco in India with the Delta variant is an example.
There is a fear that selective immune pressure by mass vaccination will churn out more variants of concern, hence there are bound to be more Delta variants. We could have very soon a Delta plus plus variant.
What could be a reasonable alternative? Ivermectin comes to mind because it blocks attachment of the virus to ACE 2 receptor. The blocking by ivermectin takes place regardless of alterations in the virus. Ivermectin does not depend upon changes in the epitopes of Covid 19 virus. It prevents binding of the virus to the ACE2 receptor, and therefore it matters little to it if there is a change in an amino acid in any protein of the virus.
Ivermectin is an extremely cheap, safe and effective generic drug available in every town of India. Covid 19 virus will be around us for many years, it is therefore incumbent on all governments to seriously consider using ivermectin as a prophylactic.
My personal clinical experience with Ivermectin has been very positive. Not a single patient for mine landed up in hospital, each began recovery within 2-3 days.
A “POSITIVE” PCR TEST DOES NOT ALWAYS INDICATE AN INFECTIVE VIRUS
On the 31st of May this year, an interesting scientific letter from German researchers was published in the ‘Journal of infection’ on the true value of a “positive” RT PCR test. The entire world now knows of the PCR test invented by Kary Mullis, who received the Nobel Prize for his invention. Importantly, the PCR test does not pick up live infective virus. It only detects genes of a virus. The German researchers have used a PCR test developed by Roche , which picks up ORF and envelope genes. They considered a cut off value of 25 cycle threshold (Ct), which is also the cut off values for home screening by the Office of National Stats (ONS) of England.
They checked more than 160000 people with the PCR test, and found 4000 positive cases. There have been 3 phases in Germany.
The mean Ct value was 27.8 in the first phase, 28.8 in the second phase and 26.6 in the third phase.
When a Ct of 25 was taken as the cut off point for infectivity, positive cases were 27% in the first phase, 27% in the second phase , and 40% in the third phase. This means that 60% to 73% of cases of positive PCR were not infective.
When a cut off of 30 Ct was taken, there were 55% positive cases in the first and second phases, while 75% were positive in the third phase, hence 25% to 45% were not infective cases.
The researchers concluded that positive PCR tests should not be taken as proof of infectivity. A positive test may simply indicate a past infection.
https://www.journalofinfection.com/article/S0163-4453(21)00265-6/fulltext?s=09#%20
The performance of the SARS-CoV-2 RT-PCR test as a tool for detecting SARS-CoV-2 infection in the population